
Arthroscopic surgical technique for tendon transfer of the lower trapezius
Técnica quirúrgica artroscópica para transferencia tendinosa del trapecio inferior
Introduction
Irreparable rotator cuff rupture (ICR) is particularly disabling when manifesting in young patients or elderly individuals that still have strong shoulder function demands, representing a genuine challenge for the orthopedic surgeon(1,2,3,4).
Tendon transfer procedures were initially reserved for patients with sequelae following brachial plexus injuries(3,5,6). This technique was subsequently extrapolated to posterosuperior ICR in the adult, with Gerber being the first to publish satisfactory middle and long term results with transfer of the latissimus dorsi (LD)(7,8). In 2016, Elhassan described the use of the lower trapezius (LT) as another option for posterosuperior ICR, citing multiple advantages versus LD(6). Finally, the arthroscopically assisted technique was described, effectively eliminating the comorbidities associated with open surgery(3).
Preoperative planning. Indications, contraindications, advantages
Before considering tendon transfer, it is important to have exhausted all the conservative management options. The ideal indication of tendon transfer corresponds to an active patient (independently of the biological age), with persistent chronic pain of the shoulder, associated to preserved passive ranges of motion and limitation of active motion, with a positive external rotation lag sign.
The imaging studies should include shoulder radiography in true anteroposterior, axillary and Y scapular projection, together with shoulder magnetic resonance imaging, in search of the following findings:
- Rotator cuff arthropathy corresponding to Hamada 1 or 2, maximum.
- Complete supra- and infraspinatus tendon rupture with fatty degeneration ≥ 3, and tendon retraction at glenoid level (Patte ≥ 3).
- Intact subscapularis tendon or with reparable damage.
The patient must show no signs of accessory spinal nerve (ASN) injury and be highly motivated for following and adhering to the postoperative recovery protocol. Lastly, it is very important for the patient to understand the postoperative expectations of a palliative surgical procedure that seeks to improve the pain and range of motion, thereby postponing the need for shoulder arthroplasty.
The contraindications of such transfer are: advanced patient age, Hamada ≥ 3 glenohumeral osteoarthrosis, deltoid deficiency, severe chronic deficiency of the subscapularis, or inability to correctly follow the postoperative protocol(1).
Among the advantages of LT with respect to other transfer procedures, mention must be made of its anatomical location of cranial origin, which affords biomechanical superiority in that it lies in line with the infraspinatus, resulting in better imitation of the force vector. It also exhibits symmetrical and in phase contraction during abduction and external rotation, which facilitates immediate adaptation and rehabilitation(9). In turn, the technique complies with all the principles of transfer in that it presents tension and excursion similar to that of the infraspinatus, potentially allowing lesser depression and anterior translation of the humeral head in the context of subscapularis insufficiency(9).
The present study describes the LT surgical tendon transfer technique, with the following modification: a double row "transosseous-equivalent" (TOE) fixation procedure using knotless bands, similar to fixation of the rotator cuff, which seeks to increase the area of contact, compression and stability of the allograft of the Achilles tendon (AT) to the greater tubercle.
Surgical technique
The surgical technique is shown in Video 1.
reacae.30279.fs2301001en-video1.png
Video 1. Video of the technique.
Positioning, location and dissection of the tendon of the lower trapezius
Under general anesthesia and brachial plexus block, with a shoulder table, the patient is placed in deck chair position, leaving the entire scapula ipsilateral to the rotator cuff lesion exposed. With patient head immobilization and the extremity to be operated upon in a TRIMANO® positioner (Arthrex), we secure stable and fixed mobility during the different phases of the operation.
The arm is to be fixed in 60-70º flexion, 20º abduction and neutral rotation in order to keep the ASN away from the medial scapular margin during location and dissection of the trapezius tendon. The sterile fields should be adequately placed on the dorsal spine, leaving its lateral zone, i.e., the zone medial to the scapular margin, free. Using a skin marker, we delimit the scapular spine and margins, alongside the line of the lateral margin of LT, which passes about 45º with respect to the scapular spine and medial margin, allowing us to palpate the subtle relief of the tendon of LT with respect to the fascia of the infraspinatus in its fossa (Figure 1).
reacae.30279.fs2301001en-figure1.png
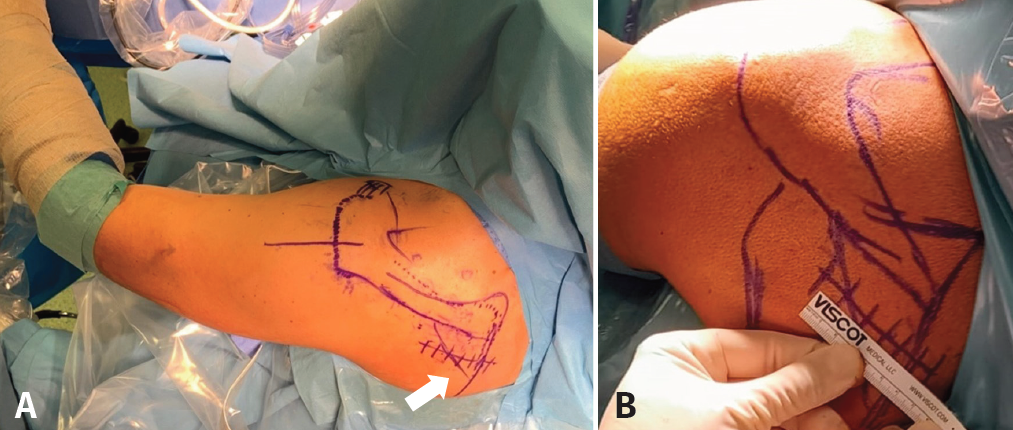
Figure 1. Left shoulder, patient placed in deck chair position, posterior view. A: the sterile fields are placed medial to the dorsal spine, leaving the space between the medial margin of the scapula and the spinous processes free. Using a skin marker, we delimit the acromion, the scapular spine, the medial margin of the scapula and the lateral border of the lower trapezius (arrow), which runs 45º with respect to the medial margin of the scapula; B: we trace the trajectory of a horizontal incision starting 2 cm medial to the medial margin of the scapula and extending 4 cm laterally, parallel to the lower border of the scapular spine.
A horizontal incision is made parallel to the inferior margin of the spine, measuring 6 cm in length and starting 1-2 cm medial to the medial margin of the scapula, with prolongation 3-4 cm in the lateral direction. We carefully dissect the subcutaneous tissue towards the adipose tissue covering the fossa of the infraspinatus, lateral to the line traced on the skin of the margin of the tendon of LT, to leave the location of its lateral margin free - this element being surprisingly thin compared with the infraspinatus. This step is crucial during the surgery, since it is here where we locate the so-called "axilla" of the tendon, thus facilitating its identification(3) (Figure 2A).
We continue along the trajectory of the tendon to its insertion in the lateral portion of the scapular spine. With a small cotton swab, we carefully dissect the plane separating LT from the fascia of the infraspinatus in the medial direction towards the medial scapular margin. An electroscalpel is used to secure complete deinsertion of the tendon of LT from its broad insertion in the uppermost margin of the spine to a maximum of 1-2 cm medial from the medial scapular margin, in order not to damage the ASN that innervates the tendon. Then, dissection is made in the inferior direction, separating the entire tendon of LT from the medial margin of the scapula, thus allowing us to palpate the rhomboid major muscle in a deeper plane. Wide opening of the fascia of the infraspinatus is made to create the entrance to the tunnel where the AT plasty (ATP) will be inserted towards the posterosuperior part of the subacromial space (Figure 2B). The obtained tendon of LT is triangular in shape, with a medial base and lateral vertex that must be reinforced with anti-tear sutures. Use is made of a less bulky flat suture, SutureTape® 1,3 (Arthrex), to prevent damage during the following traction maneuvers, especially on suturing to AT, which passes through the loop made at the center of the fine medial zone of LT (Figure 2C).
reacae.30279.fs2301001en-figure2.png
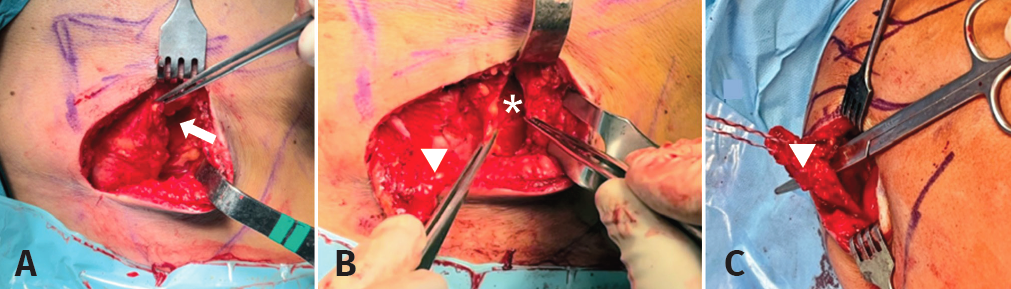
Figure 2. Right shoulder, patient placed in deck chair position, posterior view. A: we identify the axilla of the tendon of the trapezius (arrow), corresponding to the belly of the muscle separated from the fascia of the infraspinatus; B: open fascia of the infraspinatus (star) and its relation to the lower trapezius (LT)(arrowhead); C: LT with anti-tear sutures at its lateral extremity (triangle), with the scissors marking the trajectory of the loop for passing the Achilles graft according to the Pulvertaft technique.
Preparation of the Achilles allograft
This step can be carried out simultaneous to the above procedure, with the assistant surgeons. We prefer an AT allograft without bone block, measuring approximately 15-20 cm in length, as it offers an ample and robust surface for double row compression fixation to the greater tubercle.
Preparation is made with two Krackow sutures using SutureTape® 1.3 mm of a different color. We start from the narrow end, placing two entrance sutures and two exit sutures at the same end. In this way, we finally obtain four extremities of two sutures and two different colors, which facilitates identification during subacromial insertion to place each suture with the corresponding color on the medial or the lateral side of the greater tubercle (Figure 3).
reacae.30279.fs2301001en-figure3.png

Figure 3. Achilles tendon allograft prepared with Krackow sutures. Two double SutureTape® (Arthrex) sutures of different colors following entrance and exit, with the same suture color for each of the extremities.
Arthroscopy: associated lesions, preparation of the greater tubercle and tunnel for passing the Achilles plasty
The following portals are needed for this procedure: standard posterior, acromial lateral, anterolateral (AL) close to the anterior acromial angle, anteromedial (AM) close to the acromioclavicular joint, and posterosuperior (PS) near the posterior acromial angle.
From the standard posterior portal we must carefully explore the joint and rotator cuff, paying special attention to the subscapularis and long portion of the biceps (LPB). Rupture of the former always must be repaired before ATP fixation. If intact, the biceps may be preserved, performing a tenotomy and leaving it free, or knotless tenodesis taking advantage of the loop of the anterolateral implant. These procedures can be carried out with the camera in the standard posterior portal (articular) or in the PS portal (subacromial).
Debridement of the subacromial bursa is carried out, particularly of the posterior portion, to identify the space between the deltoid muscle and the remnant tendon and infraspinatus. A long Bengolea forceps loaded with a loop suture is inserted from the PS portal, with exit at the opening of the fascia of the infraspinatus, to exert traction upon the free sutures of AT and transport it from the posterior incision to the subacromial space (Figure 4A). The footprint of the greater tuberosity is routinely prepared with microfractures to facilitate the integration of AT (Figure 4B).
reacae.30279.fs2301001en-figure4.png
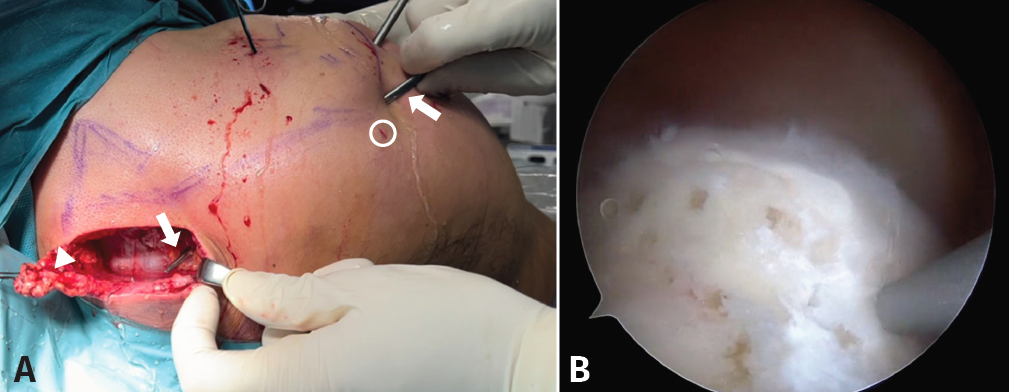
Figure 4. Right shoulder, patient placed in deck chair position, posterior (A) and intraarticular view, arthroscopic view (B). A: with the camera in the lateral portal, we see the posterior portal (white circle), as well as the Bengolea forceps showing the connection between the posterosuperior portal and the fascia of the infraspinatus (arrows), after passing through the soft physiological tunnel between the deltoid and infraspinatus (subfascial). We observe the tendon of the lower trapezius with the anti-tear stitches at its lateral end (arrowhead); B: microfractures in the footprint of the greater tubercle. Arthroscopic view from the lateral portal.
Fixation of the Achilles tendon to the greater tubercle
From the Neviaser portal, the posterior portal or PS, depending on the best angle, we place a 4.75 mm SwiveLock® (Arthrex) screw preloaded with two double sutures of different color, forming four SutureTape® 1,3 extremities in the posteromedial (PM) zone of the footprint, very close to the humeral joint cartilage. These four extremities are kept away from the footprint in the Neviaser portal in order to prevent them from interfering with the sutures of the ATP during their subacromial insertion.
Then, with the camera in the lateral portal, traction is exerted upon the suture placed with the Bengolea forceps in the PS portal to transport the Achilles sutures. At this point it is crucial to have established (at the start of surgery) the two portals AM and AL with a good angle for placing the anterior screws, so that they can be used to retrieve the suture of the extremity of the AT corresponding to its anteromedial or anterolateral end, preventing any twisting effect. Traction is exerted, displacing the tendon to the anterior portion of the footprint, immediately behind the LPB.
The second SwiveLock® screw, loaded with the medial sutures of the AT, is placed through the AM portal in the medial zone of the greater tubercle immediately behind the bicipital groove. This suture is maintained and is not cut at this point. In the same way as before, the third SwiveLock® screw is inserted from the AL portal, loaded with the lateral sutures of the AT together with the two sutures of the same color from one of the sutures of the PM screw that are set aside in the Neviaser portal. This third screw is placed in the lateral footprint of the greater tubercle posterior to the bicipital groove; the four extremities are cut immediately after fixation. In this way we secure suturing in diagonal by joining both screws, PM and AL. The loop of this third screw can be used, passing the suture from the biceps for fixation, in the event of tenodesis.
Then, the fourth and last SwiveLock® screw is placed through the PL portal loaded with the two remaining ends of the SutureTape® of the AM screw and the two remaining unused ends of the SutureTape® set aside in the Neviaser portal corresponding to the PM screw - thus completing the second diagonal suture to configure the transosseous-equivalent (TOE) fixation of the ATP. Finally, great stability with great compression of the AT is achieved (Figure 5). In this surgical phase we free the arm from the TRIMANO® positioner to exert in line traction upon the Achilles from the posterior scapular access, immediately before suturing the plasty to the trapezius, checking that the arm rotates externally.
reacae.30279.fs2301001en-figure5.png
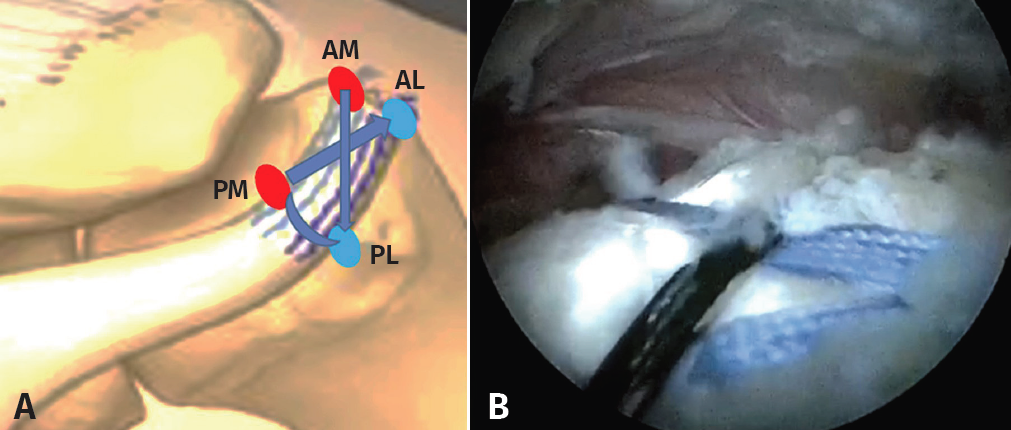
Figure 5. Final fixation of the Achilles tendon graft. A: Schematic representation of the double row transosseous-equivalent (TOE) fixation of the Achilles tendon. The red circles represent the two screws of the medial row and the blue circles those of the lateral row; B: intraarticular view showing two black tapes (SutureTape®) and two blue tapes inter-crossed diagonally, compressing the Achilles to the greater tubercle. Arthroscopic view from the lateral portal. AL: anterolateral; AM: anteromedial; PL: posterolateral; PM: posteromedial.
Fixation of the Achilles tendon to the lower trapezius and final positioning of the extremity
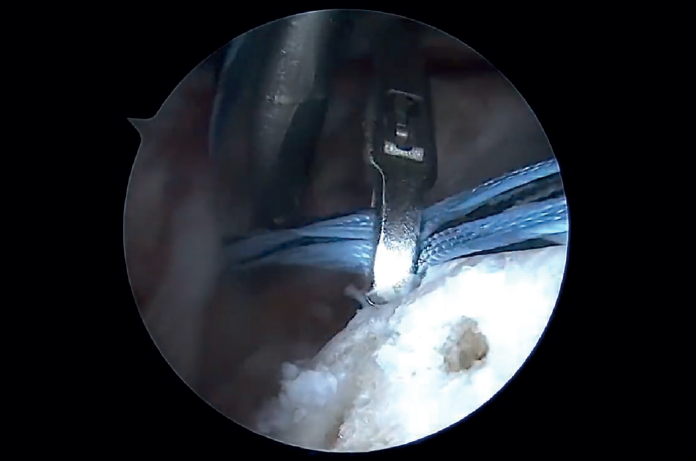
The arm is placed in 40-60º abduction and maximum external rotation. The AT is divided horizontally at its widest end in order to interlink it with the tendon of the LT based on the Pulvertaft fixation technique, ensuring the maximum possible tension during fixation with several SutureTape® 1.3 mm sutures, passed laterally through the AT and LT (Figures 6A, B and C). The posterior incision and arthroscopic portals are closed and the patient arm is placed in an immobilizer in abduction and external rotation during 6 weeks (Figure 6D).
reacae.30279.fs2301001en-figure6.png
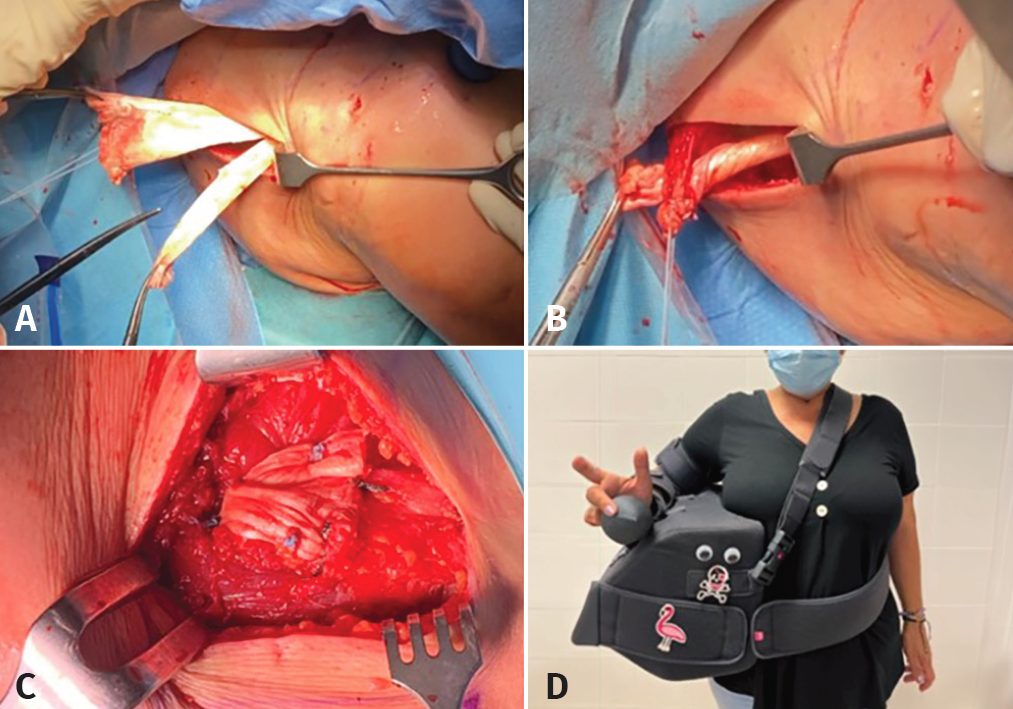
Figure 6. Right shoulder, patient placed in deck chair position, posterior view (A-C) and final view of the patient with postsurgical immobilization (D). A: a horizontal incision of the Achilles tendon graft is made at its free extremity; B-C: the free segments are interlinked one over the other to finally pass them through the loop of the lower trapezius, with fixation using non-resorbable sutures - thus connecting the Achilles tendon to the rest of the lower trapezius (LT) according to the Pulvertaft technique; D: final view of the patient with immobilization to maintain the arm in abduction and external rotation for 6 weeks.
Discussion
Irreparable rotator cuff rupture (ICR) has multiple treatment options such as simple debridement, partial repair with tenotomy / tenodesis of the LPB, superior capsular reconstruction, tendon transfers and reverse arthroplasty, as commented in this monograph. Likewise, there is a risk that improvement might not be lasting(6); agreement is therefore lacking as to which of the mentioned options is best, and no treatment of choice has been established to date(10). Posterosuperior ICR may present active external rotation loss, especially in the first degrees of abduction, associated to pain(11).
The possibility of using tendon transfers for posterosuperior ICR was first described by Gerber in 1988(12). Since then, tendon transfers have been shown to be effective in improving shoulder pain and mobility(13). These are joint preservation techniques, and like any transfer process, they require certain criteria to be met in order to secure the expected outcome: excursion and tension similar to those of the muscle being replaced; the tendon traction line must have similar strength and direction; substitution is required of a single function of the muscle being replaced; the transferred muscle must be replaceable; and finally the transferred tendon must substitute at least one degree of strength of the deficient tendon(3,6,13).
Tendon transfers of the LT using AT cadaver grafts were described by Elhassan in 2016, constituting an alternative to the use of the LD for posterosuperior ICR(4,9,12). Reddy et al. showed that the LT generates a better lever arm in that it is transferred to the footprint of the supra- and infraspinatus, compared with LD. This implies that the LT secures greater recovery of external rotation to 20º abduction of the arm. However, this advantage is eliminated at 90º abduction, where LD affords better external rotation(14). Taking into account that most daily activities requiring external rotation are performed with the arm in the first degrees of abduction, the LT appears to offer an advantage over LD. Omid et al. also showed that the LT is better able to recreate the glenohumeral kinematics and reactive forces in the shoulder(15).
One of the main disadvantages of choosing LT for ICR is the need for an allograft, with the possible drawbacks this implies: the need for access to a tissue bank, and increased surgical costs. As an alternative, Valenti has proposed using autologous tendon of the semitendinosus, thereby obviating these purported disadvantages(16). The utilization of fascia of the infraspinatus as an autograft has also been proposed, but has only been studied in anatomical models(11).
On considering the factors that can lead to a scantly satisfactory result, it has been seen that in contrast to the LD, subscapularis insufficiency, previous rotator cuff surgery, or the presence of pseudo-paralysis does not exert a significant influence when performing tendon transfer of the LT for posterosuperior ICR(9). However, the result is much better in patients that maintain active flexion of the shoulder in excess of 60º, with minimum or no shoulder osteoarthrosis, and an interval of at least two years between symptoms onset and surgery(9). There are situations in which LT transfer in posterosuperior ICR is contraindicated, such as damage to the ASN, cuff arthropathy(3), or the presence of local infection(3).
In conclusion, LT tendon transfer has been shown to be effective, reproducible and with many advantages with respect to LD transfer, though no long-term results are yet available. The AT fixation technique described in this study is carried out by means of four screws and knotless flat tape cross-interconnected to secure initial strong and stable fixation, with double row TOE compression between the AT and greater tubercle - with persistence of the weak point in healing at the allograft-tendon junction.
Conclusions
- Consensus is lacking regarding the treatment of choice for posterosuperior ICR.
- In this context, LT transfer has been introduced as a new management option with greater anatomical and biomechanical advantages, affording good clinical outcomes over the middle term.
- Tendon transfer procedures constitute palliative surgery. The patient therefore must understand and accept the reasonable expectations of such treatment.
- Adequate patient selection is essential in order to achieve a good result.
- Transfer of the LT requires a graft to reach the greater tubercle, and this constitutes a limitation of the technique.
- The use of an Achilles tendon allograft fixed with four implants and interconnected tape in double row configuration appears to increase compression and stability of the greater tubercle.
Supplementary material
The video of the technique accompanying this article can be seen at:
https://fondoscience.s3.eu-west-1.amazonaws.com/fs-reaca-videos/reaca.fs2301001-transferencia-tendinosa-trapecio-inferior.mp4
Figuras
Video 1. Video of the technique.
Figure 1. Left shoulder, patient placed in deck chair position, posterior view. A: the sterile fields are placed medial to the dorsal spine, leaving the space between the medial margin of the scapula and the spinous processes free. Using a skin marker, we delimit the acromion, the scapular spine, the medial margin of the scapula and the lateral border of the lower trapezius (arrow), which runs 45º with respect to the medial margin of the scapula; B: we trace the trajectory of a horizontal incision starting 2 cm medial to the medial margin of the scapula and extending 4 cm laterally, parallel to the lower border of the scapular spine.
Figure 2. Right shoulder, patient placed in deck chair position, posterior view. A: we identify the axilla of the tendon of the trapezius (arrow), corresponding to the belly of the muscle separated from the fascia of the infraspinatus; B: open fascia of the infraspinatus (star) and its relation to the lower trapezius (LT)(arrowhead); C: LT with anti-tear sutures at its lateral extremity (triangle), with the scissors marking the trajectory of the loop for passing the Achilles graft according to the Pulvertaft technique.
Figure 3. Achilles tendon allograft prepared with Krackow sutures. Two double SutureTape® (Arthrex) sutures of different colors following entrance and exit, with the same suture color for each of the extremities.
Figure 4. Right shoulder, patient placed in deck chair position, posterior (A) and intraarticular view, arthroscopic view (B). A: with the camera in the lateral portal, we see the posterior portal (white circle), as well as the Bengolea forceps showing the connection between the posterosuperior portal and the fascia of the infraspinatus (arrows), after passing through the soft physiological tunnel between the deltoid and infraspinatus (subfascial). We observe the tendon of the lower trapezius with the anti-tear stitches at its lateral end (arrowhead); B: microfractures in the footprint of the greater tubercle. Arthroscopic view from the lateral portal.
Figure 5. Final fixation of the Achilles tendon graft. A: Schematic representation of the double row transosseous-equivalent (TOE) fixation of the Achilles tendon. The red circles represent the two screws of the medial row and the blue circles those of the lateral row; B: intraarticular view showing two black tapes (SutureTape®) and two blue tapes inter-crossed diagonally, compressing the Achilles to the greater tubercle. Arthroscopic view from the lateral portal. AL: anterolateral; AM: anteromedial; PL: posterolateral; PM: posteromedial.
Figure 6. Right shoulder, patient placed in deck chair position, posterior view (A-C) and final view of the patient with postsurgical immobilization (D). A: a horizontal incision of the Achilles tendon graft is made at its free extremity; B-C: the free segments are interlinked one over the other to finally pass them through the loop of the lower trapezius, with fixation using non-resorbable sutures - thus connecting the Achilles tendon to the rest of the lower trapezius (LT) according to the Pulvertaft technique; D: final view of the patient with immobilization to maintain the arm in abduction and external rotation for 6 weeks.

Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors state that they have no conflicts of interest.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their work centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- Sometimes the rotator cuff injury of the shoulder is not repairable and we will have to do something with it…
- More manuscripts!
- Teach everything, tell everything
- Irreparable massive ruptures of the posterosuperior cuff: definition, diagnosis and classification
- Conservative management with medication and other non-surgical invasive therapies
- Physiotherapy and electrophysical therapies in the conservative management of irreparable posterosuperior rotator cuff rupture
- Alternatives in irreparable ruptures of the posterosuperior cuff. Debridement, tenotomy, partial repair
- Surgical alternatives in irreparable ruptures of the posterosuperior cuff
- Tendon transfers in irreparable ruptures of the posterosuperior rotator cuff. Latissimus dorsi and lower trapezius
- Reverse replacement in a patient without osteoarthritis
- Arthroscopic surgical technique for tendon transfer of the lower trapezius
- Arthroscopy assisted latissimus dorsi transfer for irreparable posterosuperior rotator cuff injuries really works
- Instructions for authors (Sept. 2023)
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.