
Reverse replacement in a patient without osteoarthritis
Prótesis inversa en paciente sin artrosis
Introduction
Irreparable cuff ruptures are difficult to treat and are often associated with uncertain outcomes(1). These are usually chronic and retracted lesions characterized by atrophy and adipose infiltration of muscle(2,3,4,5,6). Affected patients typically visit the clinic due to pain and functional impairment, with loss of strength and mobility, and even pseudo-paralytic shoulder, with an elevation of less than 90º in the absence of stiffness(7,8). In other cases, mobility is preserved and the main complaint is pain(9).
Although there are different definitions of massive cuff rupture(10,11,12,13,14), the two most widely used approaches are based on the dimension of tendon rupture (> 5 cm)(11,12) and on the number of affected tendons - with a minimum of two(4,13,14).
Different treatment options have been presented in this monograph, though the fact is that there is no solid evidence of the clear superiority of any given treatment over the rest. When in addition to massive cuff rupture the patient presents glenohumeral arthropathy, there is considerable agreement that many of the therapeutic options addressed in this monograph would not be indicated. In this scenario, reverse replacement is the treatment that proves most predictable in affording pain relief and the recovery of function, with an increase in quality of life of these patients(15,16,17,18).
A more controversial issue is its indication in patients with massive cuff rupture in the absence of arthropathy, since it implies performing joint replacement of a joint without osteoarthrosis. In these cases, reverse shoulder replacement has been shown to be an effective alternative that affords predictable pain relief and improved function(15,17) (Figures 1 to 5).
reacae.30279.fs2212027en-figure1.png
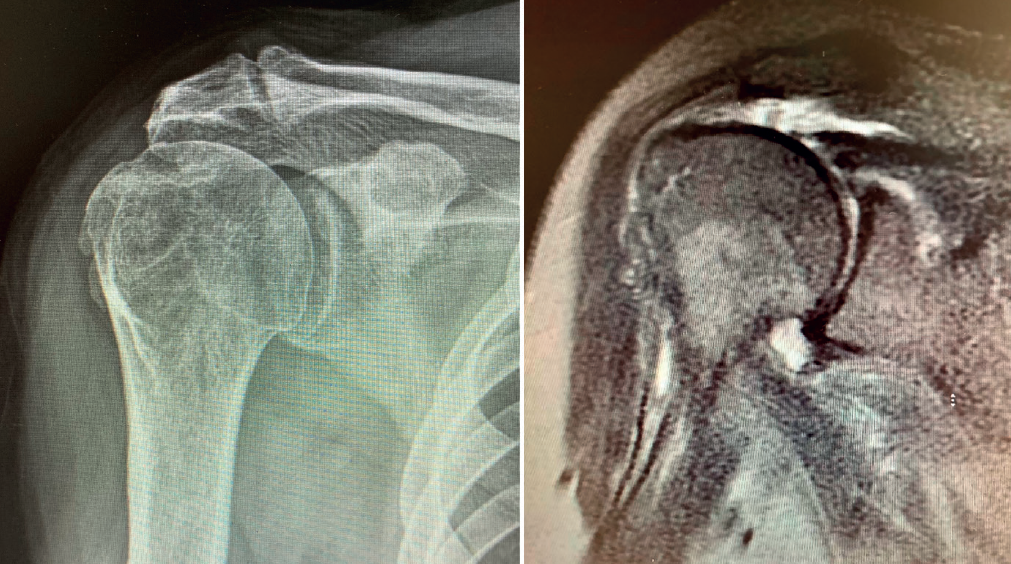
Figure 1. Preoperative anteroposterior radiographic view of a patient with massive rupture without osteoarthrosis, and coronal magnetic resonance imaging view of the same patient, showing massive cuff rupture corresponding to grade 3 of the Patte classification, in a 68-year-old male.
Reverse shoulder replacement shifts the center of rotation distal and medial (Figure 5), increasing the lever arm of the deltoid muscle and recruiting more anterior and posterior fibers of the muscle, improving its function in patients without rotator cuff(1,19,20). In general, the patients can be expected to show increased anterior flexion and abduction of the shoulder. Having greater or lesser external rotation will depend on the quality of the teres minor and infraspinatus, among other factors (Figure 4). With regard to internal rotation in patients with reverse shoulder replacement after massive rupture, the results are less predictable and are conditioned by the implant design and the characteristics of the patient, among other factors. We must know the functional limitations of the implant and inform our patients about the results that can be expected.
reacae.30279.fs2212027en-figure2.png

Figure 2. Sagittal view of massive cuff rupture in a 68-year-old male, affecting three tendons (subscapularis, supra- and infraspinatus) and measuring over 5 cm.
The aim of the present literature review is to describe the current indications, the results, and survival and complications of reverse replacement procedures in patients with massive cuff rupture in the absence of arthropathy.
Outcomes of reverse arthroplasty
In the case of a patient with irreparable massive cuff rupture in the absence of osteoarthrosis, surgical treatment would be indicated if there is significant pain and/or important functional impairment that have failed to improve with adequate orthopedic management.
Because of the difficulties of achieving correct repair in these patients, the high repeat rupture rate and the unpredictability of the outcomes, many surgical alternatives to "standard" repair have been proposed for situations of this kind. Such techniques have been addressed in the course of this monograph (partial repairs, tenotomy of the long portion of the biceps, subacromial balloon, capsule reconstructions, transfers, etc.). To date, there are no solid scientific data allowing a clear preference for any one of these techniques, and we must individualize the treatment strategy in each concrete patient.
reacae.30279.fs2212027en-figure3.png
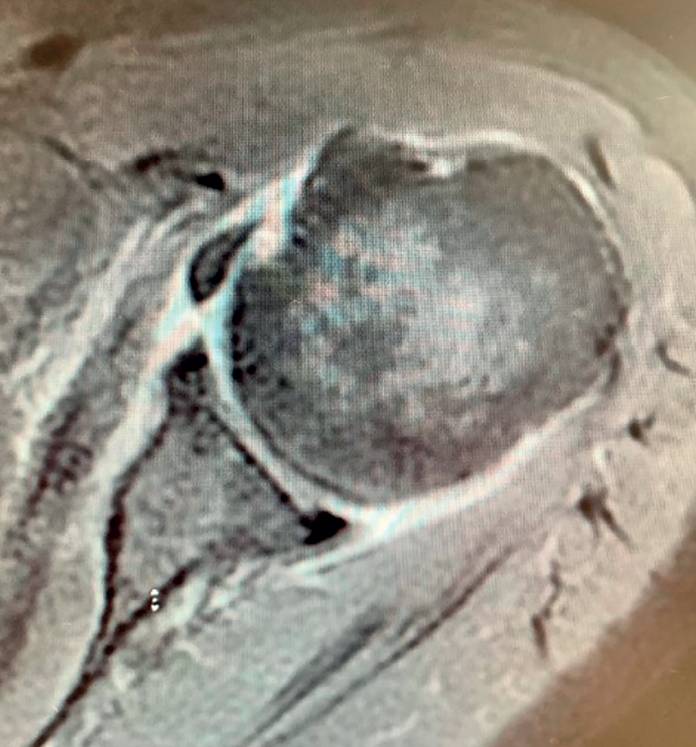
Figure 3. Axial view of massive cuff rupture in a 68-year-old male, showing complete and retracted rupture of the subscapularis.
There is another alternative for the treatment of irreparable massive cuff rupture in patients without osteoarthrosis: reverse shoulder replacement, which affords predictable pain relief and improved function in these individuals.
Practically all of the consulted literature and also the personal experience of the author coincide that irreparable cuff rupture remains a genuine challenge for the shoulder surgeon, particularly in young patients without arthropathy.
reacae.30279.fs2212027en-figure4.png
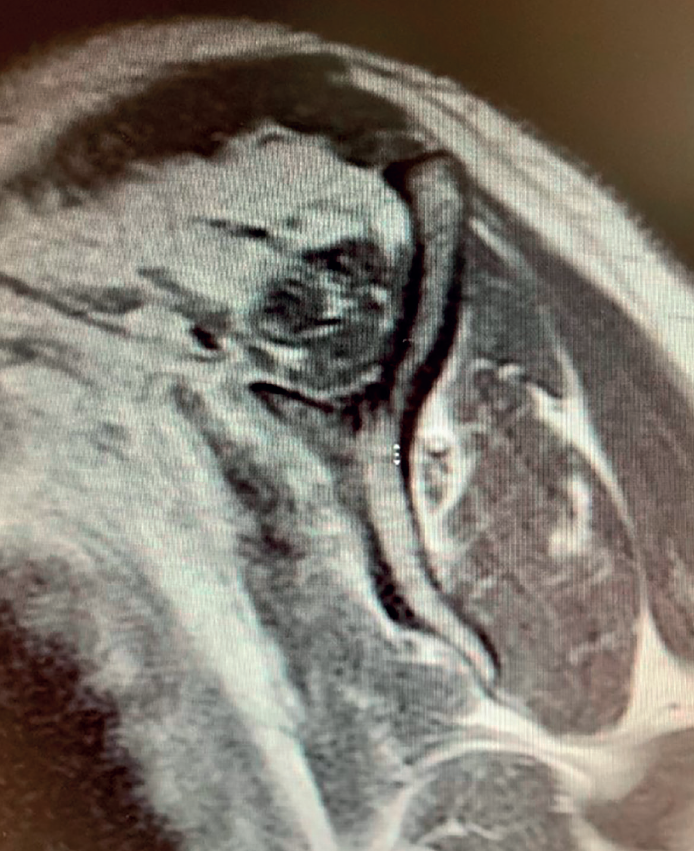
Figure 4. Sagittal view of massive cuff rupture in a 68-year-old male, showing grade 3 adipose muscle degeneration of the supraspinatus, with grade 2 degeneration of the infraspinatus and subscapularis according to the classification of Goutellier.
In older patients or individuals with glenohumeral arthropathy, there is strong agreement in the literature that reverse replacement is a safe option that is very useful for treating massive cuff ruptures and arthropathy due to cuff rupture. This type of surgery has been shown to afford shoulders with a good range of motion and function without pain, and moreover improves the scores on the different functional scales.
reacae.30279.fs2212027en-figure5.png

Figure 5. Anteroposterior radiograph of the shoulder of a 68-year-old male with reverse replacement surgery due to massive rupture of the rotator cuff. Onlay reverse implant with section at 135°, uncemented stem 75 mm in length, and 39 mm glenosphere. Very good clinical outcome.
Many studies have assessed the outcomes of reverse replacement in patients with arthropathy, though much less information is available on patients with massive cuff rupture in the absence of arthropathy.
In 2017, S. Petrillo published a systematic review(21) with the evaluation of over 400 patients with reverse shoulder replacement due to cuff rupture, and involving a mean follow-up period of 35 months. The study concluded that reverse replacement improved anterior flexion, abduction and external rotation (flexion 73.4°, abduction 74.3°, external rotation in adduction 10.6° and external rotation in 90° abduction 28.5°) - the values recorded being statistically significant.
In 2017, Sevivas, in another systematic review(1) involving 266 shoulders subjected to reverse replacement, concluded that the latter significantly improved the outcomes (pain, function and mobility) in patients with irreparable rotator cuff ruptures.
The indication of reverse replacement in patients with arthropathy due to cuff rupture thus seems clear. However, in younger active patients without arthropathy, the indication of reverse replacement is more controversial, due to the high complications rate involved. Furthermore, the high patient activity levels, concerns about implant longevity, and the high complication rates of revision surgery are added issues in this scenario(15,22,23).
Authors such as Ek, Muh, Samuelsen, Hartzler, Frankle or Ernstbrunner(15,17,24,25,26,27) have reported excellent results with reverse replacement surgery in patients suffering massive cuff rupture without arthropathy, with follow-up periods ranging from 2-12 years.
In 2013, Muh(24) reported that 81% of the patients under 60 years of age subjected to reverse replacement due to irreparable cuff rupture were very satisfied or satisfied after 36.5 months, with significant improvement of pain and the functional scores.
Likewise, Samuelsen reported a high patient satisfaction rate (90%) and improvement of the functional scores and pain in patients under 60 years of age after three years of follow-up(25).
It also must be taken into account that in the studies of Muh and Samuelsen, the indications of reverse replacement surgery included arthropathy due to cuff tearing, failed primary total shoulder arthroplasty and rheumatoid arthritis. However, despite these different indications and the fact that the present review focuses on patients with massive cuff rupture in the absence of arthropathy, it is very useful to know the results, risks and complications of reverse replacement in active patients under 60 years of age.
In 2018, Frankle also recorded significant improvement of the outcomes in 92 patients with reverse replacement due to massive cuff rupture without arthropathy, and involving a minimum follow-up of two years(26).
We can also find long term studies of reverse shoulder replacement in young patients. In 2017, Ernstbrunner(27) described the long term results over an average follow-up of 11.77 years after reverse replacement in 23 patients under age 65 with irreparable cuff rupture. This author reported subjective and objective clinical improvement that persisted after 12 years.
Ek(15) reviewed 46 reverse replacements in patients under 65 years of age with pseudo-paralysis due to massive cuff rupture with or without osteoarthrosis. Good results were obtained, with improvements of over 40% on the Constant scale, and no differences were observed with respect to patients that had undergone previous surgery. However, Muh(24) reported poorer outcomes in patients that had undergone previous surgery, in a population group very similar to that of Ek.
Complications of reverse arthroplasty
Reverse shoulder replacement therefore offers a very good alternative for the management of massive cuff ruptures without arthropathy in a group of patients that may be regarded as young, with reliable outcomes that seem to be maintained over the years. Nevertheless, due consideration is required of the high complications rate in these individuals, ranging from 17% to 39%, and the need for revision surgery in up to 17% of the cases. On the other hand, these rates were recorded in specialized centers where the surgeons had experience with reverse replacement surgery; the complication rates therefore could be even higher in less experienced hands.
In their systematic review published in 2017 and involving over 400 reverse replacements (including massive ruptures and patients with cuff rupture arthropathy), Petrillo(21) recorded clinical improvement on all the functional, mobility and pain scales, though with a complications rate of 17.4% - the most frequent problem being heterotopic ossification (6.6%), stress fractures of the scapula or acromion (3%), luxation (1.2%) and infection (1%). Furthermore, up to 7.3% of the patients required revision surgery, especially due to loosening of the components, mechanical failure, luxation and infection.
In 2013, Muh(24), in his study on reverse replacement in patients under 60 years of age, reported a complications rate of 15% - the most frequent problem being luxation, followed by infection.
In addition, although the mobility and functional scores were similar to those obtained in other series involving more older patients (in the study by Muh the mean age was 52 years), the patient satisfaction levels and subjective criteria proved less favorable in this group of individuals, probably due to greater expectations regarding the outcome in the young patients.
In coincidence with Muh, Ek(15), in his series of 46 patients under 65 years of age, recorded a complications rate of 37.5% (15 patients), with luxation in 7 individuals and infection in 5 - though only 6 of the 15 patients required implant replacement.
In 2017, Ernstbrunner(27) documented a complications rate of 39%, a revision surgery rate of 17% and a failure rate of 9%, in 23 patients under age 65.
In turn, in 2015, Hartzler published a retrospective study of 74 cases of reverse shoulder replacement in patients with massive rupture without glenohumeral arthropathy in which the outcomes in terms of mobility, function and pain were very satisfactory, but with a complications rate of 17% over a minimum follow-up of two years. The authors identified patient age (< 60 years), a high preoperative functional score (Simple Shoulder Test [SST] > 7) and neurological dysfunction (axillary or brachial plexus) as independent risks factors for poorer outcomes(17).
Although infection and luxation are the complications with the greatest impact upon the patient, other complications of a mechanical kind may result from the non-anatomical design of the reverse replacement implant. Anterior impingement with the coracoid process may be responsible for limited internal rotation, while posterior impingement limits external rotation. Impingement of the greater tubercle with the acromion may also occur, limiting abduction. Inferomedial impingement causes friction with the lower part of the scapula during rotation and adduction (so-called scapular notching), which can result in wear of the polyethylene and bone erosions(28). Lastly, and also as a consequence of the non-anatomical design of the reverse replacement implant, the medial displacement of the center of rotation caused may produce instability by reducing soft tissue tension(28).
Apart from the complications that may arise when indicating reverse shoulder replacement, we must know and inform the patients about the limitations of this arthroplasty: the internal and external rotation we can expect after reverse replacement (especially in the absence, rupture or adipose infiltration of the teres minor) is often limited(29). Boileau(30,31) showed that if the patient presents a deficit in external rotation associated to massive cuff rupture without arthropathy, we will only be able to restore external rotation through tendon transfer.
Boileau in 2005 or Simovitch in 2007(28,32) concluded that reverse replacement is unable to secure the restoration of external rotation. In many patients, only the teres minor will be able to afford active external rotation. If the teres minor presents rupture, retraction or adipose degeneration (which can be assessed by magnetic resonance imaging or computed tomography), we can predict a poorer outcome in these individuals, with an external rotation deficit(33,34). The lack of external rotation may prove quite disabling, especially in patients that use the arm in abduction. For this reason, some investigators such as Longo, in 2011(35), indicate the possibility of latissimus dorsi transfer to the reverse replacement implant, to restore external rotation in the patient.
Grammont in 1993(20) and subsequently Boileau in 2005(28) proposed increasing humeral retroversion of the reverse implant to improve external rotation.
Authors such as Gulotta(36) or Stevenson(37) conducted biomechanical studies and showed that placing the humeral stem in 20º or 20-40º of retroversion increases external rotation without humeroscapular conflicts.
On the other hand, both Boileau and Gramont(20,28) reported that improved internal rotation can be obtained if the stem is placed in anteversion.
In 2017, Petrillo et al.(21) compared the functional outcomes of patients with reverse shoulder replacement with the stem at 30º and at 10-20º of retroversion; flexion and abduction proved greater in the patients with the stem at 10-20º of retroversion, and external rotation in the patients with 30º of retroversion. These differences were not statistically significant, however.
In their meta-analysis, Petrillo et al.(21) showed reverse replacement to afford very good results in terms of clinical and functional parameters (Constant score, pain, function, etc.), but less so in relation to external rotation. In fact, Hartzler(17) found that the subgroup of patients with transfer of the latissimus dorsi experienced greater gain in external rotation, concluding that reverse arthroplasty may be more effective in improving pain than mobility.
Before indicating reverse shoulder replacement in a patient with massive cuff rupture without arthropathy, we must consider the possibility of obtaining good results with cuff suture, tendon transfer, or any of the other techniques described in this monograph. In 2022, Bei Liu(38) compared suture and reverse replacement in patients with massive cuff rupture without arthropathy. Both options were found to be effective and reliable in treating massive rupture without arthropathy. However, shoulder function was seen to be better in the repair group; hence, repair should be seen as the first treatment choice in these patients. However, it must be taken into account that the follow-up period was two years and that the patients had massive but repairable ruptures, since repair proved possible in all the patients of the suture group, with a 36% repeat rupture rate (which is totally acceptable in the context of massive rupture repairs).
Considering the risks and alternatives, despite the potential clinical improvements after reverse replacement in younger patients with irreparable cuff ruptures, we must be cautious in considering this procedure in a young and active patient - given the high complications rate and the known technical challenges associated with revision surgery of reverse shoulder replacement(39).
Implant longevity is another important concern in young patients. In a population with a mean age of 73 years, Favard(40) showed that the Constant score dropped from 88% to 78% in 5 years. As early as 2006, Guery(41) had published similar results on the evolution of function with reverse replacement surgery, with a survival rate of 58% at 10 years.
Neither Favard nor Guery(40,41) found a clear explanation for the functional deterioration over time; radiolucency or scapular notching could be implicated, though it has not been possible to confirm this.
Although as seen in this article there have been authors such as Ek or Ernstbrunner(15,27) who have reported high survival rates after more than 10 years with reverse replacement in patients under 65 years of age, it must be clear to us that the main objective in the management of massive cuff rupture in younger patients is to preserve the shoulder rather than contemplating arthroplasty.
Conclusions
Reverse shoulder replacement affords excellent, reliable, reproducible and lasting outcomes in patients with massive cuff rupture without arthropathy, though the complications rate can be high. Adequate patient selection is required, with due consideration of our experience in reverse replacement procedures and the management of their potential complications and revision surgeries.
Figuras

Figure 1. Preoperative anteroposterior radiographic view of a patient with massive rupture without osteoarthrosis, and coronal magnetic resonance imaging view of the same patient, showing massive cuff rupture corresponding to grade 3 of the Patte classification, in a 68-year-old male.

Figure 2. Sagittal view of massive cuff rupture in a 68-year-old male, affecting three tendons (subscapularis, supra- and infraspinatus) and measuring over 5 cm.
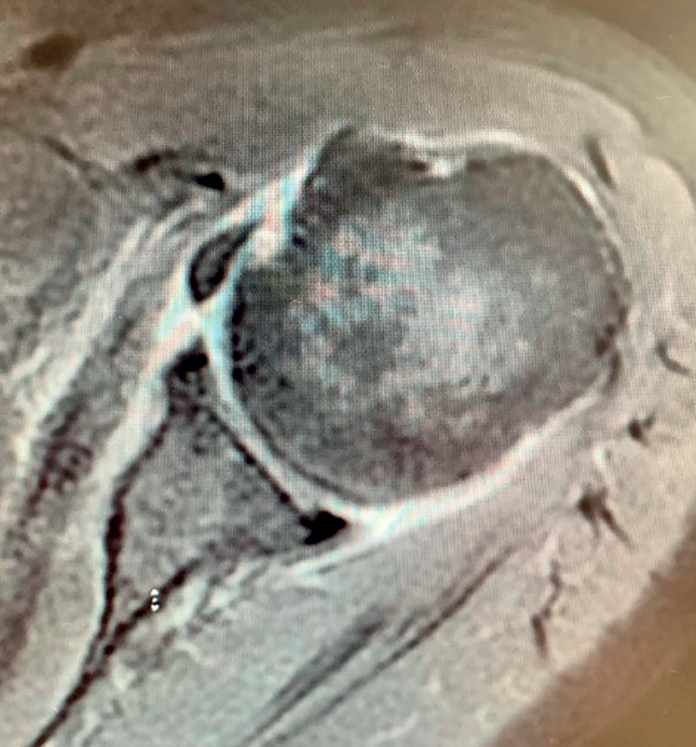
Figure 3. Axial view of massive cuff rupture in a 68-year-old male, showing complete and retracted rupture of the subscapularis.

Figure 4. Sagittal view of massive cuff rupture in a 68-year-old male, showing grade 3 adipose muscle degeneration of the supraspinatus, with grade 2 degeneration of the infraspinatus and subscapularis according to the classification of Goutellier.

Figure 5. Anteroposterior radiograph of the shoulder of a 68-year-old male with reverse replacement surgery due to massive rupture of the rotator cuff. Onlay reverse implant with section at 135°, uncemented stem 75 mm in length, and 39 mm glenosphere. Very good clinical outcome.

Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors state that they have no conflicts of interest.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their work centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- Sometimes the rotator cuff injury of the shoulder is not repairable and we will have to do something with it…
- More manuscripts!
- Teach everything, tell everything
- Irreparable massive ruptures of the posterosuperior cuff: definition, diagnosis and classification
- Conservative management with medication and other non-surgical invasive therapies
- Physiotherapy and electrophysical therapies in the conservative management of irreparable posterosuperior rotator cuff rupture
- Alternatives in irreparable ruptures of the posterosuperior cuff. Debridement, tenotomy, partial repair
- Surgical alternatives in irreparable ruptures of the posterosuperior cuff
- Tendon transfers in irreparable ruptures of the posterosuperior rotator cuff. Latissimus dorsi and lower trapezius
- Reverse replacement in a patient without osteoarthritis
- Arthroscopic surgical technique for tendon transfer of the lower trapezius
- Arthroscopy assisted latissimus dorsi transfer for irreparable posterosuperior rotator cuff injuries really works
- Instructions for authors (Sept. 2023)
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.