
Anatomical ligament reconstruction with allograft in chronic acromioclavicular dislocations restores joint stability and function. Short-term outcomes in 14 cases
La reconstrucción ligamentosa anatómica con aloinjerto en luxaciones acromioclaviculares crónicas restaura la estabilidad articular y permite recuperar la función. Resultados a corto plazo en 14 casos
Introduction
Traumatic injury to the acromioclavicular joint is frequent and affects young and active individuals(1). Mild acute lesions (types I and II of the Rockwood classification) are subjected to conservative management, with good results(2). In the case of more serious injuries (Rockwood types III, IV and V), surgery is considered much more often(2,3,4,5). Nevertheless, conservative management is effective in many cases, and there is a clear tendency to adopt this approach and to offer surgery only in those cases characterized by persistent clinical manifestations following a variable period of conservative treatment(6). This strategy is justified by the acceptable outcomes of surgery in the management of such lesions in the subacute or chronic phase(7,8).
Many techniques are used for the treatment of chronic dislocations of the acromioclavicular joint(9), and there are no clear indications as to which technique is best. Since the primary healing capacity of the coracoclavicular ligaments (CCLs) beyond three weeks is limited(10), dislocations with an evolution longer than this can be regarded as non-acute, and some type of biological augmentation becomes necessary. In general terms, the alternatives are divided into non-anatomical techniques, that modify the normal anatomy using the coracoacromial ligament or the coracobrachialis to substitute the affected ligaments, and anatomical techniques based on the use of autologous, allogenic or artificial tendon grafts to reconstruct the ligaments. Although historically the techniques used were focused on management of the CCLs, it now seems to have become clear that the acromioclavicular ligaments (ACLs) are also crucial. As a result, anatomical techniques that restore both ligament complexes and repair the trapezoid-deltoid fascia are becoming the option of choice for the management of these lesions(11,12,13).
The present study was carried out to analyse the short-term radiological and functional outcomes of an anatomical technique that reconstructs the acromioclavicular and coracoclavicular ligament complexes with the help of a tendon allograft for the management of acromioclavicular dislocations with an evolution of over three weeks.
Methods
A prospective longitudinal study was made of a series of cases with subacute or chronic acromioclavicular dislocations treated by one same surgical team using a technique involving reconstruction of the CCLs and ACLs with the help of a posterior tibial allograft. The study was approved by the Ethics Committee of the Hospital Universitario Ramón y Cajal (Spain). All patients gave their consent to participation in the study.
Patients
The study included all patients with subacute or chronic acromioclavicular dislocations (over three weeks of evolution) requiring surgical management due to persistent symptoms after acute injury. The patients were operated upon by three senior shoulder surgeons from one same team in three both public and private hospitals.
The inclusion criteria were: 1) age over 18 years; 2) type III, IV or V acromioclavicular injury according to the Rockwood classification, with an evolution of over three weeks; and 3) persistent symptoms (pain or functional limitation) despite conservative management.
The exclusion criteria were: 1) acute lesions; 2) type I or II injury according to the Rockwood classification; 3) presence of associated lesions of the pectoral girdle (fractures or dislocations); and 4) previous surgery of the mentioned joint.
Surgical technique
The surgical technique reproduces that presented by Kibler et al. in 2017(12) and referred to by these authors as the MADOK technique. The technique has been described in detail in an additional article(14), but is summarized here. A longitudinal incision is made over the distal third of the clavicle, in line with its major axis, to expose the acromioclavicular joint. The ruptured ACLs are identified and separated (they almost always remain inserted in the acromion). An anterior or posterior tibial tendon allograft is prepared, measuring 15 cm in length and 5 mm in thickness. The coracoid process is identified and a passage beneath it is prepared with a dissector. Two orifices measuring 5 mm in diameter are made craniocaudally in the clavicle over the insertional footprint of the conoid and trapezoid ligaments. The acromioclavicular joint is reduced and temporarily fixed with a Kirschner wire. The graft is passed through each of the orifices and beneath the coracoid process; reinforcement is provided by four passes of high-resistance polyethylene tape (UltraTape®, Smith & Nephew, Boston, USA) displaced adjunct to the graft beneath the coracoid process, with knotting over the distal surface of the clavicle. Both ends of the allograft are sutured together over the clavicle and are placed over the acromioclavicular joint. Two sutures are passed through two 2-mm tunnels on the dorsal side of the acromion, and the ends of the tendon are sutured to these sutures over the lateral bone bridge. The ACLs are reinserted over the distal clavicle with the help of two all-suture implants measuring 1.7 mm (SutureFix® 1.7 mm, Smith & Nephew, Boston, USA). We repair the trapezoid-deltoid fascia over the reparation and the temporary fixation pin is removed. Resection of the distal clavicle is not carried out; in the case of evident deformity due to osteophytes, shape smoothing is performed.
Following surgery, all patients were immobilized with a 20° abduction sling during four weeks (to facilitate recovery of glenohumeral abduction), allowing its removal for active exercises of the elbow and hand, and for passive shoulder flexion exercises. Pendular exercises were explicitly to be avoided. During weeks 5 to 8, the orthosis was suspended and assisted active mobility exercises were started. Free active mobility was allowed in week 9, though strengthening exercises were postponed until 90% of the normal range of motion was achieved. An exercise program was then started, focused on the recovery of normal scapulothoracic kinetics.
Clinical and radiological evaluation
Prior to surgery, the epidemiological data were collected and all patients were evaluated using the Constant-Murley, American Shoulder and Elbow Surgeons (ASES)-shoulder and Quick-DASH (Disabilities of the Arm, Shoulder and Hand) scales. We measured the coracoclavicular distance in the healthy shoulder and the affected shoulder from plain anteroposterior radiographs, tracing a vertical line from the upper part of the coracoid process to the lower surface of the clavicle(15).
After surgery, the intraoperative complications were recorded. Likewise, the coracoclavicular distance and size of the clavicular tunnels were measured from the postoperative radiographs. Reduction was considered to be adequate when there was no increase in the coracoclavicular distance of over 25% with respect to the contralateral side.
The patients were evaluated one year after surgery and on a yearly basis thereafter. Use was made of the Constant-Murley, ASES-shoulder and Quick-DASH scales (the scores were standardized to a scale of 0-100, where 100 = perfect functional outcome). The presence of complications over follow-up was also documented. Based on the plain radiographs, we recorded the coracoclavicular distance in the affected shoulder, widening of the tunnels, and the presence of fractures or osteolysis of the distal clavicle. Likewise, careful exploration of the reconstructed joint and of the scapulothoracic kinetics was carried out(12), with palpation of the joint in search of pain in response to pressure or crepitation. We palpated the distal clavicle and acromion in search of signs of subtle instability in the superoinferior and anteroposterior planes, establishing comparisons with the healthy side. The joint was inspected during flexion and abduction movements of the arm in order to assess its dynamic stability. Any appearance of increased translation in either of the two planes was recorded. We visually analysed the presence of static and dynamic scapular asymmetries during active flexion of the shoulder(16).
Statistical analysis
Normal distribution of the quantitative variables was assessed using the Kolmogorov-Smirnov test. These variables were reported as the mean-standard deviation (SD), and the Student t-test for paired samples was used for comparison purposes. Statistical significance was considered for p < 0.05.
Results
The MADOK technique was applied to a total of 19 patients between January 2015 and January 2020. Two subjects were excluded: one presented malunion of an associated fracture of the middle third of the clavicle, and corrective osteotomy was performed at the same time, while the other patient had undergone surgery for acromioclavicular instability on three previous occasions. Thus, the inclusion criteria were finally met by 17 subjects, of which 14 (82%) were available for evaluation an average of 2.7 (1.1) years after surgery (range 14 months - 5 years).
reacae.28373.fs2102004-figure1.png
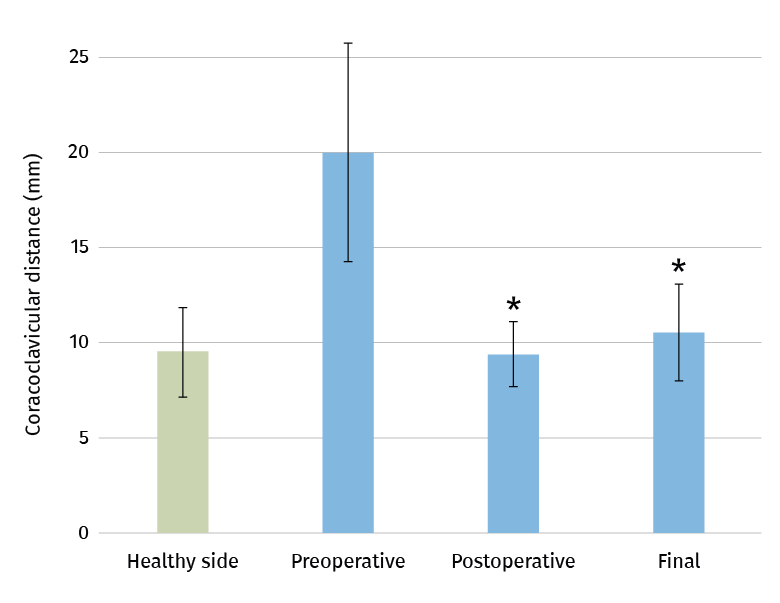
Figure 1. Coracoclavicular distance measured from the anteroposterior radiograph of the shoulder. The data correspond to the affected side (preoperative) and the healthy side as reference. The described technique allowed recovery of normal coracoclavicular distance after surgery (postoperative) and at the end of follow-up (final). * Significant differences (p < 0.0001) with respect to the preoperative values. There were no significant differences among the postoperative, final and healthy side values.
The epidemiological, clinical and radiological data of the 14 finally included patients are reported in Table 1. The degree of craniocaudal displacement of the affected clavicle with respect to the contralateral clavicle is shown in Figure 1. Fresh frozen tibial tendon allografts measuring 5 mm in diameter were used in all the procedures, and 5-mm tunnels were made in the distal clavicle. There were no perioperative or immediate postoperative complications.
reacae.28373.fs2102004-table1.png
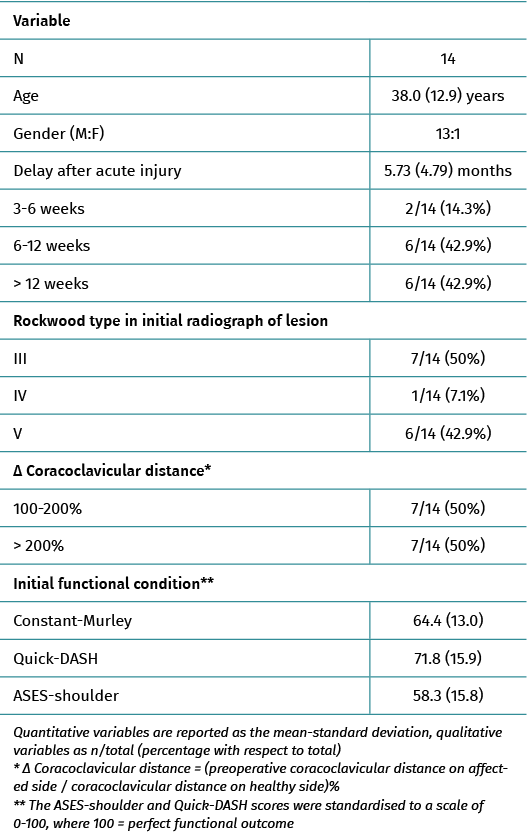
Table 1. Epidemiological, clinical and radiographic characteristics of the study series
The postoperative radiographic control evidenced correct reduction of the joint, with a restored coracoclavicular distance in 12 patients (85.7%); two subjects presented insufficient reduction but which was considered acceptable (43% and 54% increase in coracoclavicular distance).
reacae.28373.fs2102004-table2.png
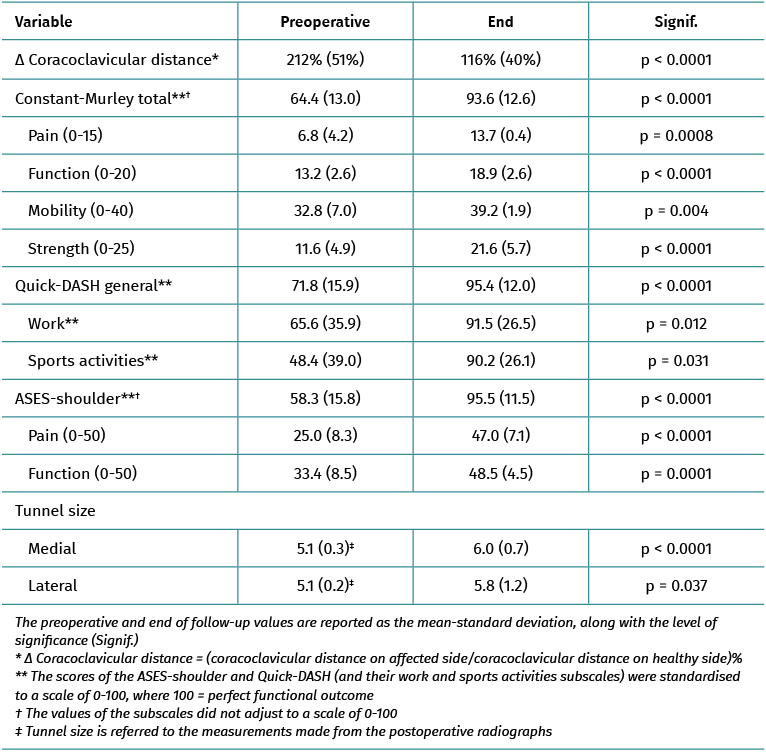
Table 2. Clinical and radiological outcomes of the study series
At the end of follow-up, significant improvement was observed in all three functional assessment scales and their sub-sections (Table 2 and Figure 2). Thirteen patients (93%) presented distal clavicular stability in both planes at exploration, with no noticeable scapulothoracic dyskinesia. The good reduction achieved in the immediate postoperative period in 12 of the 14 patients persisted at the end of follow-up, though the degree of displacement in the two subjects with insufficient correction in the postoperative period was seen to progress (with increments of 74% and 132%, respectively). In addition, we documented osteolysis of the distal clavicle and mild degenerative changes in the acromioclavicular joint in 5 cases. With regard to the size of the clavicular tunnels, an increase in diameter was noted, though the increase was only > 2 mm in three tunnels corresponding to three different individuals.
reacae.28373.fs2102004-figure2.png
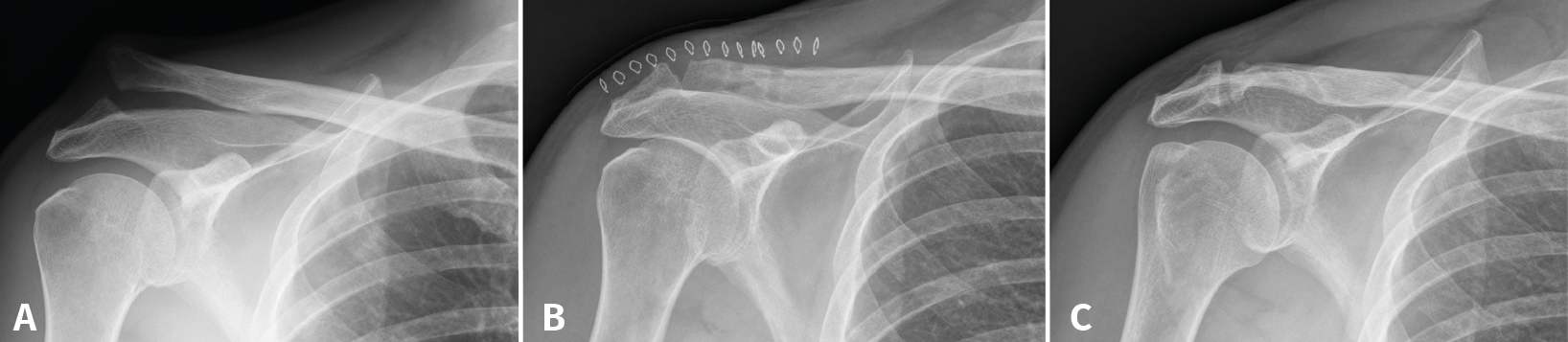
Figure 2. An 18-year-old male presenting type V acromioclavicular dislocation initially subjected to conservative management. One year after the injury he presented persistent symptoms and absolute limitation for sports activities (A). Surgery was performed with good reduction of the deformity (B), and four years after the operation the functional outcome was excellent (C), with minimum degenerative changes in the acromioclavicular joint and some widening of the clavicular tunnels.
The two patients in which initial correct reduction of the joint was not achieved were seen to group most of the complications. The first patient, a 52-year-old woman with type IV acromioclavicular dislocation operated upon after four weeks of pain and dysfunction refractory to conservative management, presented insufficient reduction (54% displacement), progressive loss of reduction (finally 132%) and a poor functional outcome 14 months after surgery (Constant-Murley = 54; Quick-DASH = 69; ASES-shoulder = 57) - with evident scapular dyskinesia and clear anteroposterior and craniocaudal instability of the distal clavicle (Figure 3). The patient declined any other additional procedures. The second patient, a 50-year-old man with type V acromioclavicular dislocation subjected to conservative management during four months without success, presented initially insufficient reduction (43%) with progressive loss of reduction (74% at the end of follow-up), osteolysis of the distal clavicle and widening of the proximal orifice of the clavicle to 7.7 mm. These findings nevertheless had no functional repercussions, since after 18 months of follow-up the functional outcome was very good (Constant-Murley = 94; Quick-DASH = 88; ASES-shoulder = 99).
reacae.28373.fs2102004-figure3.png
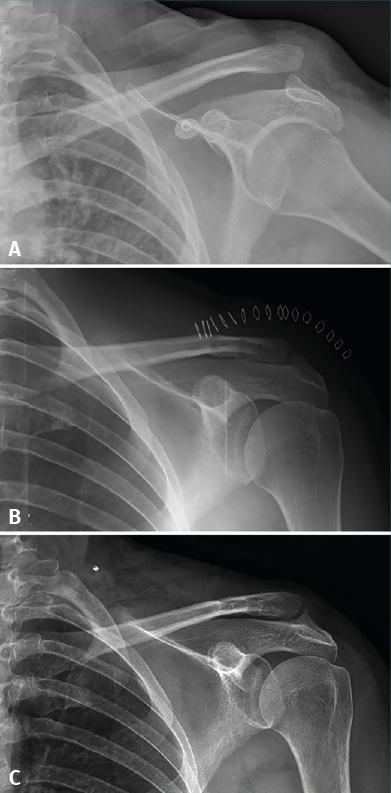
Figure 3. A 52-year-old woman with type IV acromioclavicular dislocation (A) subjected to surgery four weeks after injury due to refractory pain and dysfunction. The surgical outcome was considered acceptable, though with insufficient reduction (B). Fourteen months after surgery, the patient suffered persistent symptoms and loss of reduction was seen to have progressed (C).
Discussion
The main finding of this study is that the MADOK technique for reconstruction of the CCLs and ACLs with allografts is effective in restoring stability and function in patients with chronic acromioclavicular dislocations. Good correction of the instability is achieved during the surgical procedure, and consistent outcomes are obtained 2.7 years after the operation, without relevant complications.
There is much controversy as to which technique is best for the management of chronic acromioclavicular instabilities. In the same way as in other disorders, there are innumerable technical variants. In general terms, the surgeon should take three decisions into account: whether to perform an anatomical reconstruction of the joint and its ligaments, or use a non-anatomical technique; whether to use a graft as an adjunct to the soft tissues; and, if so, whether to use an autologous, allogenic or artificial graft. All these options have their advocates, who very recently have published excellent results(17,18,19,20).
Two systematic reviews have been published in 2020 that allow some light to be shed on this issue. Borbas et al.(21) conducted a meta-analysis of 27 studies involving 590 patients, comparing the outcomes of anatomical techniques with artificial grafts, anatomical techniques with tendon grafts, and non-anatomical techniques. The authors concluded that while the outcomes were similar, the studies of greater methodological quality were favourable to the anatomical techniques with grafts. On the other hand, Sircana et al.(13) carried out a meta-analysis of 44 studies involving over 1000 patients, and came to the conclusion that anatomical reconstructions (with either biological or artificial grafts) afforded the best results. It must be taken into account that the real differences in outcomes were small among the different techniques, and that all the evaluated procedures had similar complication rates and offered good results.
The outcomes obtained in the present series are similar to those reported by other authors using anatomical techniques to reconstruct both ligament complexes with grafts. Kibler et al.(12), in the initial description of the MADOK technique, recorded good results in 15 patients followed-up on during three years, with restoration of stability in both planes, no residual dyskinesia, and only one case of loss of reduction with a poor functional outcome. Saccomanno et al.(11), using a very similar technique including a tunnel in the acromion through which the autograft was passed, obtained good results in 30 patients followed-up on over an average of two years. Loss of reduction of the acromioclavicular joint was observed in four cases, but this did not appear to have an important functional impact. The only poor outcome in this series was related to a lack of reduction of the joint in the immediate postoperative period; precise intraoperative assessment of reduction should always be carried out.
In the present series widening of the clavicular tunnels was regularly observed over follow-up, though no relevant functional effect was noted. Berhold et al.(22) also observed such widening without functional repercussions in a review of 24 patients with three years of follow-up, though Sircana et al.(13) in their meta-analysis recorded clavicular fractures associated to the tunnels in 0.7% of the subjects subjected to biological reconstructions with grafts. It cannot be ruled out that this may represent a problem that was not evidenced in our series due to the limited number of patients involved.
Lastly, the outcomes in the present series can be regarded as excellent. This has certain implications in the acute management of severe acromioclavicular dislocations: conservative strategies become more relevant, since deferred surgery affords results similar to those of surgery in the acute phase, as suggested by the systematic review published by Song et al.(7). Such reasoning is fundamented not only upon this study - which has its limitations - but also on the data obtained with this technique by Muench et al.(8), who found the expected outcomes of the surgical treatment of such chronic lesions to be similar to those obtained in patients in whom initial conservative management proved effective.
Limitations
The present study has two important limitations: firstly, the number of included patients is limited, and this may cause infrequent complications (such as the aforementioned clavicular fractures) to go unnoticed. Nevertheless, the sample size does allows us to identify the improvements obtained on the functional scales as being significant and clinically relevant. Secondly, the duration of follow-up was insufficient. Although all patients were evaluated at least one year after surgery, the clinical outcomes could possibly worsen over longer periods of time. In particular, the presence of degenerative changes in the acromioclavicular joint observed in the radiographic studies at the end of follow-up appeared to have no functional repercussions, though in view of the young age of the patients, such changes might have consequences over the long term. In turn, it should be noted that among the individuals with correct initial reduction, no worsening at all was observed in the quality of reduction after 2.7 years of follow-up. Lastly, the clinical case series design of our study poses limitations compared with other studies that include a control group.
Conclusions
Satisfactory short-term outcomes were obtained with this anatomical technique that reconstructs the acromioclavicular and coracoclavicular ligament complexes with the help of a tendon allograft for the management of acromioclavicular dislocations with an evolution of over three weeks. In this small case series, the technique was seen to be safe, with no complications.
Figuras
Figure 1. Coracoclavicular distance measured from the anteroposterior radiograph of the shoulder. The data correspond to the affected side (preoperative) and the healthy side as reference. The described technique allowed recovery of normal coracoclavicular distance after surgery (postoperative) and at the end of follow-up (final). * Significant differences (p < 0.0001) with respect to the preoperative values. There were no significant differences among the postoperative, final and healthy side values.
Figure 2. An 18-year-old male presenting type V acromioclavicular dislocation initially subjected to conservative management. One year after the injury he presented persistent symptoms and absolute limitation for sports activities (A). Surgery was performed with good reduction of the deformity (B), and four years after the operation the functional outcome was excellent (C), with minimum degenerative changes in the acromioclavicular joint and some widening of the clavicular tunnels.
Figure 3. A 52-year-old woman with type IV acromioclavicular dislocation (A) subjected to surgery four weeks after injury due to refractory pain and dysfunction. The surgical outcome was considered acceptable, though with insufficient reduction (B). Fourteen months after surgery, the patient suffered persistent symptoms and loss of reduction was seen to have progressed (C).
Tablas
Table 1. Epidemiological, clinical and radiographic characteristics of the study series
Table 2. Clinical and radiological outcomes of the study series
Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors state that they have no conflicts of interest.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that the procedures carried out abided with the ethical standards of the responsible human experimentation committee and in accordance with the World Medical Association and the Declaration of Helsinki.
Data confidentiality. The authors declare that the protocols of their centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors have obtained informed consent from the patients and/or subjects cited in the article. The mentioned document is filed by the corresponding author.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- Don’t forget to remember
- Anatomical study on subtalar arthrodesis: anterolateral versus posterior portals
- Customized 3D printed guides for the repair of rupture of the posterior root of the internal meniscus. Preliminary outcomes
- Anatomical ligament reconstruction with allograft in chronic acromioclavicular dislocations restores joint stability and function. Short-term outcomes in 14 cases
- Patellar tendinopathy: diagnostic approach and functional assessment scales
- Current management of posterior cruciate ligament rupture. A narrative review
- Management of anterior instability of the shoulder with bone defects
- Open anatomical reconstruction surgical technique with allograft for the treatment of chronic acromioclavicular dislocations
- Simultaneous but different damage to both posterior meniscus roots with multiple ligament injury of the knee following high-energy trauma. Presentation of a case
- Pigmented villonodular synovitis of the ankle
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.