

Rehabilitation following anterior capsulolabral arthroscopic Bankart repair: a guide for the young arthroscopist
Rehabilitación tras reparación capsulolabral anterior de Bankart artroscópica: una guía para el artroscopista joven
Introduction
Rehabilitation following repair of the anterior capsulolabral complex of the shoulder contemplates progressive recovery of shoulder function while also protecting capsule-ligament healing. The rehabilitation protocol should be adapted to the characteristics and pattern of instability, and to the factors inherent to the patient and the injury. Patient age, the characteristics of rupture (size, position, quality of the tissue), the associated lesions (glenoid or humeral bone loss, osteochondral lesions) and confidence in surgical fixation can affect the progression of rehabilitation(1).
Patients with anteroinferior relapsing glenohumeral instability present weakness of the internal and external rotators of the shoulder(2), which affects the dynamic stability of the joint. The relationship between muscle weakness and anterior instability has been well documented(3) and is important in the origin and evolution of the disease, independently of the anatomical lesions that may appear following the instability episodes. In the case of anterior capsulolabral repair, this muscle weakness is compounded by capsule stiffness that may occur as a consequence of the surgical procedure(4). The importance of postoperative rehabilitation is that it constitutes the main tool for progressively correcting this dynamic instability while also preventing the development of joint stiffness after the operation.
The ultimate aim of rehabilitation should be the restoration of normal function of the operated shoulder. In this respect, two main lines of intervention have been defined: on one hand the recovery of glenohumeral and scapulothoracic mobility, and on the other hand reinforcement of the rotator cuff and periscapular musculature in order to improve neuromuscular control of the joint(4). However, the published protocols offer no clear evidence regarding the recovery phases or the movements or exercises that should be avoided in each step(1). Consequently, there is often confusion as to how to address the rehabilitation of a shoulder subjected to anterior capsulolabral repair and the timelines that should be followed.
The present study describes a basic rehabilitation scheme, divided into three phases, with the aim of helping young arthroscopists in their decision making, and of reviewing the available evidence on the recommendations made.
An interventional protocol divided into three chronological phases is described and developed: a first protection phase in which the main aim is pain control and protection of the repaired structures; a second active recovery phase seeking to restore active mobility and reinitiate basic activities of daily living; and a third functional recovery phase, with the resumption of physical exertion similar to that performed before the operation. It is important to underscore that there should be no strict timelines for these phases, since the duration of each period must be individualized according to the characteristics of each patient. Nevertheless, a series of concrete periods will be established in an attempt to define approximate time limits between each phase.
First phase: protection
In the early period of rehabilitation (from the immediate postoperative period to week 6, approximately), the main aim is to protect capsulolabral healing and reduce the pain and inflammation. The secondary objectives include protected mobilization of the joint and the start of scapulothoracic muscle strengthening.
The first aim is to afford adequate analgesia, both in the immediate postoperative period and once the patient has returned home. In addition to improving patient comfort, this will contribute to ensure adequate adherence to the instructions provided, and thus improve the final outcome(5).
The most important aspects of early rehabilitation are detailed below.
1. Immobilization
Following surgical repair, healing of the capsulolabral structures requires appropriate stress to stimulate repair while also affording protection against excessive tension. The gradual application of stress constitutes a stimulus for fibroblast proliferation and differentiation. Over time, the repaired tissues gradually increase their resistance to traction. Traditionally, patients subjected to capsulolabral repair surgery were fully immobilized with a sling during 6 weeks(6). Different studies have shown that immobilization for shorter periods of time does not increase the instability recurrence rate(7,8). Despite these findings, however, most published studies and clinical guides continue to recommend immobilization for 4.8 ± 1.8 weeks(9).
There is no scientific evidence on the adequate position of immobilization following Bankart repair surgery. The use of an external rotation (ER) sling as conservative treatment after a first episode of anterior shoulder dislocation was popularized by Itoi(10), though posteriorly Whelan et al.(11) published a meta-analysis of 6 clinical trials in which no differences were found between the two types of immobilization. None of these studies mention the position of the sling following anterior capsulolabral repair, however; no clear recommendations can therefore be made in this regard.
2. Mobility
In this stage we start to work upon passive mobility while protecting the surgical repair.
In the same way that excessive loading is deleterious for the integrity of the surgical repair, controlled passive or assisted active weight bearing can contribute to tissue healing. During the early postoperative period we should indicate exercises with restricted and progressive motion ranges that are safe and that protect the repair(12). Most of the published guides focus on gaining joint mobility and elasticity - limiting the specific range of motion of each evolutive stage. It is important to mention that such progression must always be adapted to the tolerance of the patient; we must not move on to a greater range of motion if pain does not allow the patient to reach the minimum objectives.
reaca.28272.fs2006035en-figure1.png
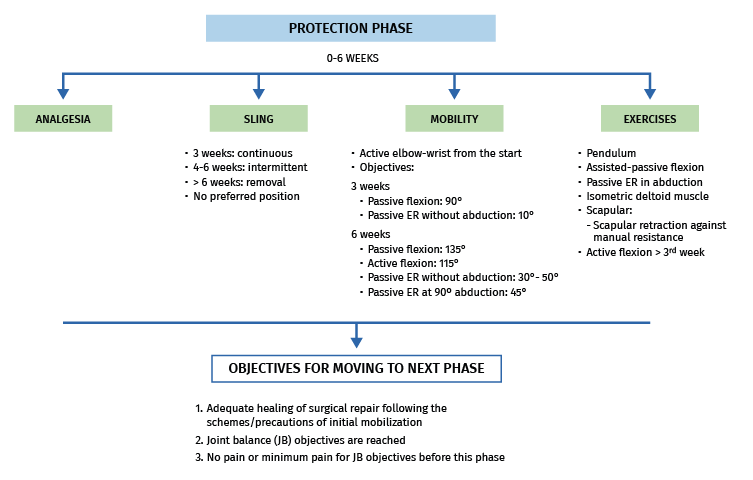
Figure 1. Most important aspects during the protection phase.
In 2010, the American Society of Shoulder and Elbow Therapists developed a consensus document specifying a series of stepwise increase in motion objectives during the postoperative period of anterior Bankart repair surgery (Figure 1) as a guide for patients and therapists(13). Stepwise increase in motion objectives have been shown to be very useful for achieving adequate progression of motion, thanks to the stimulus which the defining of a time limit represents for the patient(7). These objectives in turn can be modified according to the characteristics of each individual and the preferences of the surgeon. If the objectives are not reached within the established time period, gentle passive mobilization by physiotherapists is indicated. In contrast, if the objectives are reached too quickly, the established safety limits should not be exceeded, in order not to tension the repaired structures more than necessary, taking into account that anterior flexion exposes the lower part of the joint capsule to tension, in the same way that ER tensions the anterior capsular tissues while internal rotation (IR) tensions the posterior capsular tissues.
3. Exercises
During this stage the exercises detailed below will be described to the patient, keeping the extremity in the sling for the rest of the time in order to avoid excessive use of the arm, which could place the surgical repair at risk. All the exercises should be performed without pain and minimizing the number and magnitude of repeated weight bearing. There are no differences between the home exercise programs and the hospital rehabilitation programs in patients subjected to capsulolabral repair surgery(14); it is therefore advisable to individualize each case and adapt each program to the needs of each individual.
reaca.28272.fs2006035en-figure2.png
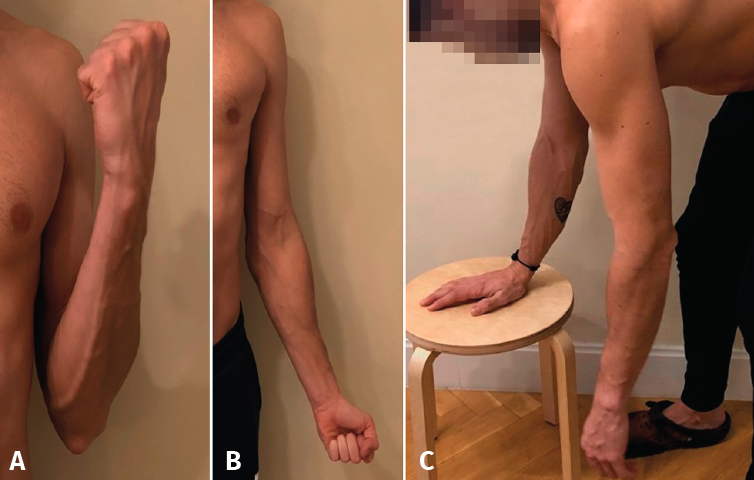
Figure 2. A: active elbow flexion exercise; B: active elbow extension exercise; C: Codman pendulum exercise.
Day 1 - 3 weeks
• From the time of surgery the patient should be instructed to perform flexion-extension of the elbow (Figures 2A and 2B), wrist and hand. The aim on one hand is to avoid elbow stiffness problems as a consequence of immobilization, and on the other hand to improve pain control.
• Pendulum exercises. We can choose between the following:
1. Codman pendulum exercise (Figure 2C), in which the patient bends forwards, flexing the trunk, and with the contralateral forearm resting on a table or chair, while the affected arm is swayed trying to minimize muscle activity around the glenohumeral joint. As the patient progresses, we can include weights of between 1.5-2.5 kg, likewise without muscle activation.
2. Chandler pendulum exercise, in which the patient lies in prone decubitus on the stretcher with the affected arm outside the stretcher, performing the pendular movement.
reaca.28272.fs2006035en-figure3.png

Figure 3. Isometric exercises of the deltoid muscle.
• Isometric cuff exercises without exceeding 90° of flexion and 10° of ER without abduction. Isometric exercises of the deltoid muscle (Figure 3) are complementary during the early phase. The starting position is with the arm in adduction, with the elbow flexed 90° and with neutral ER. We instruct the patient to perform flexion, abduction and extension without producing movement, and keeping the deltoid muscle contracted for 5 seconds.
• Elevation exercises. There are four types of elevation exercises which our patients can perform: pulley-assisted elevation exercises, elevation exercises assisted with the contralateral arm in decubitus, bar-assisted elevation exercises, and step-back exercises on the table (Figures 4A
and 4B).
• External rotation exercises. The physiotherapist performs passive mobilizations in ER at 0° of abduction and without exceeding 10°. In addition, the patient may perform the same exercise with the help of a bar, always controlling neutral positioning of the shoulder (Figure 5A).
• Scapular exercises: during this stage we should start exercises seeking to correct malpositioning of the scapula during the range of motion. Scapular retraction exercises are made without loading and under controlled extension of the shoulder (Figure 5B), with progression to scapular retraction exercises against manual resistance.
reaca.28272.fs2006035en-figure4.png
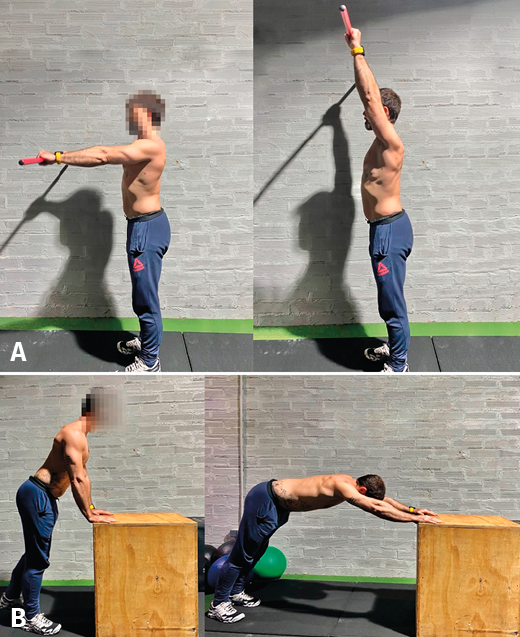
Figure 4. A: passive elevation exercise with bar; B: step-back passive elevation exercise with table.
Weeks 3-6
In this phase we start to progressively remove the sling during the day, and we complete the exercises that should have started in the previous weeks. The timeline objectives described in Figure 1 must be taken into account. If any of the aforementioned exercises could not be done before because of poor tolerance, they can now be introduced in this phase.
Figure 1 summarizes the most important aspects that apply during the protection phase.
Second phase: active recovery
Once the protection phase has been completed, we assume that healing has been effective; more aggressive exercises can therefore be introduced, maintaining protection of the repaired structures.
reaca.28272.fs2006035en-figure5.png
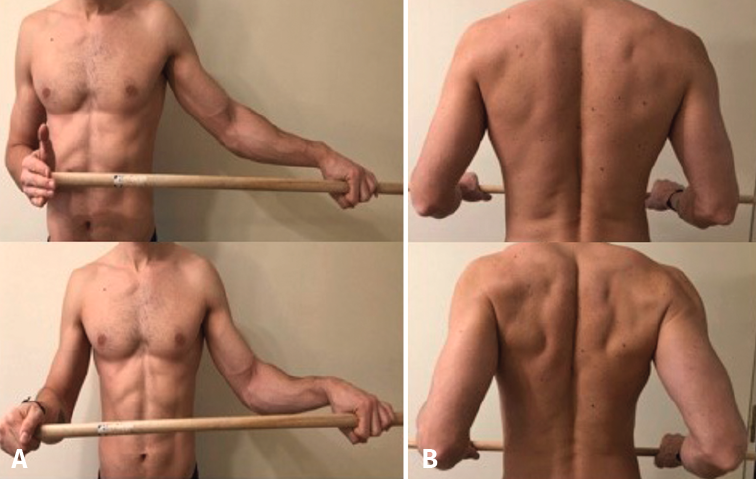
Figure 5. A: passive external rotation exercise with bar; B: scapular retraction exercise.
The primary objectives in this period (approximately from week 7 to week 12 after surgery) will be the complete recovery of active joint balance and the correction of scapular dyskinesias and muscle imbalances - including the strengthening of joint proprioception. The secondary objective is to start to gain muscle strength.
The following specific interventions apply during this period:
1. Main activities:
a. Continuous patient education on use of the upper extremity: how to avoid lifting heavy objects, rapid and sudden movements, or positions that exert tension upon the anteroinferior capsule.
b. Assisted active / passive motion, as required to reach (without exceeding) the established joint balance objectives.
c. Exercise of the rotator cuff and scapular neuromuscular control within the allowed balancing range.
2. Complementary activities:
a. Introduction of functional movement patterns.
b. Progressive resistance exercises.
The global exercises that should be avoided in this stage are:
• Do not perform stretching beyond the joint balance objectives.
• Do not perform stretching to gain ER in the last degrees or at 90° of abduction(12).
• Do not allow the patient to use the arm to lift heavy objects.
• Do not perform strengthening exercises involving heavy loading of the shoulder in horizontal abduction or in combined abduction with ER (e.g., push-ups)(15).
• Do not perform abduction of the scapular plane with IR.
Mobility
Continuing with the scheme referred to gain in joint range proposed in the section above, based on the recommendations of the American Society of Shoulder and Elbow Therapists, the motion objectives over the following weeks are described in Table 1(13).
reaca.28272.fs2006035en-table1.png
Table 1. Mobility objectives during the active recovery phase.
The main novelty in this stage is that we must work both passive and active mobility in all planes - always according to patient tolerance and following a logical progression, without exceeding the proposed time limits. We often only require light stretching exercises(16). If mobility falls significantly short of the established objectives, physiotherapist intervention will again be needed to perform gentle passive mobilizations. However, these exercises should be made only in the directions that are limited, and only until the established objectives have been reached(17).
Muscle re-education
In this stage we need to intensify correction of the anomalous motion patterns caused by scapular dyskinesia. Such correction should have already started in the protection phase through the aforementioned scapular exercises, though at this point we place much more emphasis on this aspect.
The aim is to correct scapular malpositioning during motion of the upper extremity. Anterior instability gives rise to attenuation of the anterior capsular tissue due to irreversible plastic deformation that often accompanies disinsertion of the anteroinferior labrum. This anatomical alteration results in deficit of the dynamic stabilizers, scapular malpositioning during shoulder movements and - ultimately - a loss of the cavity-compression effect exerted by muscle activation during the medium ranges of motion(18,19). In addition to this, mechanoreceptor alteration occurs as a consequence of surgery itself.
reaca.28272.fs2006035en-figure6.png
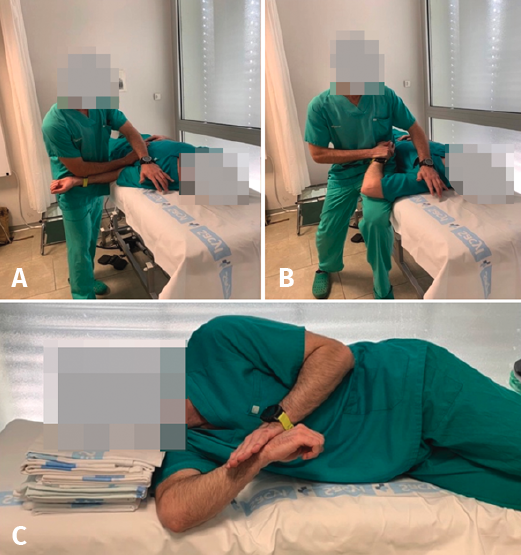
Figure 6. A: pectoralis minor assisted stretch exercise; B: internal rotation assisted stretch; C: sleeper stretch.
The fundamental static alteration is an inclination towards scapular protraction, which causes displacement of the humeral head outside the centre of the glenohumeral joint(20). The position of the scapula in protraction is favoured by a decrease in activation of the subscapular, inferior trapezius and anterior serratus muscles, as well as an increase in the activation of the pectoralis minor and latissimus dorsimuscles(21). The rehabilitation program should seek to allow work with the scapula in retraction, where activation of the periscapular muscles is more effective(22,23). This should be done in a controlled and progressive manner, always protecting the surgical repair, based on the following exercises:
1. Stretching and mobilization techniques. It is important to identify the less flexible structure in order to centre our work on specific muscle groups(24):
- Flexibilization of the pectoralis minor (Figure 6A):
- Shoulder abduction at 90° in ER and elbow at 90° in corner / angle.
- Assisted passive stretch, moving the scapula to the posterior pivot and retraction position, with the shoulder in neutral elevation position while ER is performed.
- Contracture of the posterior capsule:
- Assisted IR stretches in the supine position, shoulder in abduction and manual stabilization of the scapula (Figure 6B).
- Sleeper stretch exercises (Figure 6C): the patient in lateral decubitus performs self-assisted passive IR with the shoulder at 90° of flexion.
- Cross arm stretch: the patient performs self-assisted passive shoulder adduction at 90° of anterior flexion of the shoulder.
reaca.28272.fs2006035en-figure7.png
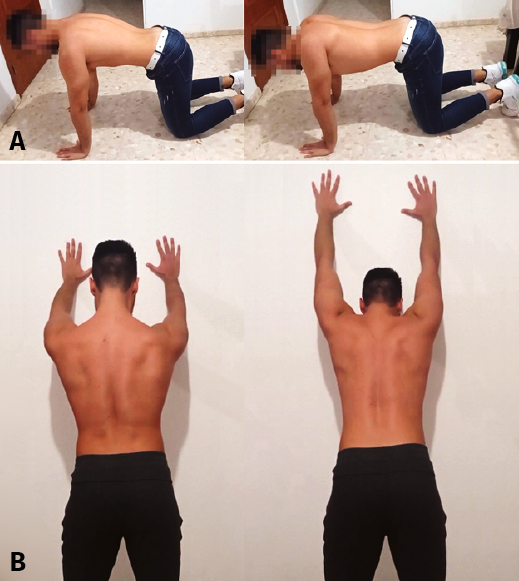
Figure 7. A: anterior serratus exercise on all fours; B: anterior serratus exercise in standing position.
2. Work on periscapular muscle and proprioceptive control:
- Basic "closed chain" movement and postural exercises in front of the mirror, with physiotherapeutic correction.
- Loading exercises with a fixed distal segment, e.g., from on all fours, the patient works to maintain the adequate position of the scapula, or scapular protraction is performed progressing to the tripod position, without flexions(25,26,27) (Figures 7A and B).
3. Specific muscle strengthening to correct dyskinesia. These exercises should begin once an acceptable motion range has been achieved.
Figure 8 summarizes the most important actions for the correction of dyskinesia during Bankart surgery rehabilitation.
reaca.28272.fs2006035en-figure8.png
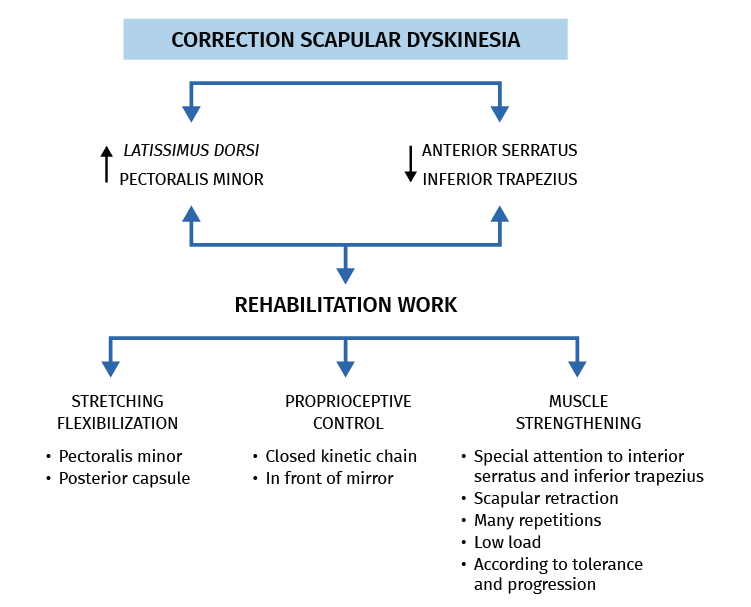
Figure 8. Measures destined to correct scapular dyskinesia following arthroscopic anterior capsulolabral repair.
Muscle strength
Once the protection phase has been completed, and in addition to the already described isometric exercises to strengthen the deltoid muscle, we can introduce exercises to strengthen the periscapular muscles(28). As a general rule, we should avoid exercises involving excessive loads and plyometric exercises in this phase.
• The exercises should be performed in a comfortable position with low stress of the glenohumeral joint, such as elevation of under 45° in the scapular plane. We can start without weight in prone decubitus or in lateral decubitus(29).
• The elevation activities can progress from assist exercises (e.g., rope and pulley, walking along the wall) to vertical exercises against resistance.
• Almost complete active elevation in the scapular plane should be achieved before moving on to other planes.
• The increase in anterior capsule tension should be gradual, working towards an elevated ER position in the coronal plane.
• The speed of the exercises should be gradually increased according to patient tolerance. In general, slower speeds are indicated in repetitions of the open kinetic chain exercises.
• The rotator cuff and strengthening of the scapular stabilizers exercises should place emphasis on numerous repetitions (commonly 30-50 repetitions) and relatively low resistance (typically 1-2 kg)(30).
• Strengthening of flexo-extension of the elbow with the arm at the side can begin in this phase, always starting with elastic elements (e.g., elastic bands) and in a shoulder adduction position.
reaca.28272.fs2006035en-figure9.png

Figure 9. A: low row strength exercise; B: lawnmower strength exercise.
A broad range of exercises have been described that comply with the above premises. Ideally, these exercises should combine work on muscle strength with muscle re-education. The following exercises are described due to their simplicity and reproducibility, though they do not have to be performed on an exclusive basis:
• Low row exercise: the patient moves to scapular retraction from the initial position of the scapula with extension of the trunk. Modifications of this exercise, with unilateral support on the ipsilateral leg or bilateral support with the ipsilateral leg in an advanced position allow us to implicate the entire kinetic chain during the exercise (Figure 9A).
• Lawnmower movement from inferior adduction with the arm extended to abduction of the shoulder with the elbow flexed (Figure 9B).
• Exercises sliding the arm resting on the wall, performing closed chain work.
• Rowing exercises in the standing position, in different controlled flexion-abduction degrees of the shoulders.
Figure 10 summarizes the most important aspects of the active recovery phase.
reaca.28272.fs2006035en-figure10.png
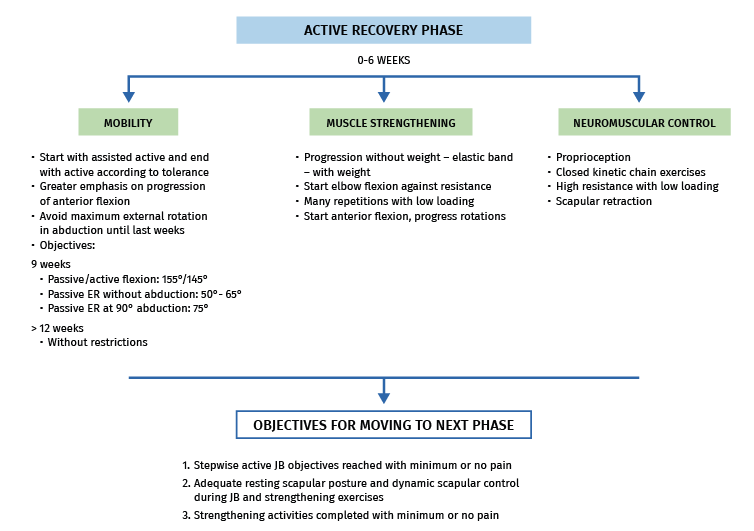
Figure 10. Most important aspects during the active recovery phase.
Third phase: functional recovery
Approximately week 12 after surgery is considered to be the point for starting physical exertion activities, since at this time the dynamic stabilizer strength defect is less than 15% - provided the rehabilitation program has been carried out satisfactorily(31). This means that at this time the shoulder will have enough strength to start activities involving greater physical demands(32,33), without neglecting protection of the surgical repair. In this regard, the repair scar will continue to mature and undergo remodelling until 40 or 50 weeks after the operation, following a process analogous to Wolff's law in bone repair(34,35).
In this phase individualization according to the objectives of each patient becomes even more necessary, depending on the leisure or occupational activities we wish to achieve. Although the patients have similar characteristics at the start of this phase of the rehabilitation process, the endpoint may be quite different. There are specific programs for athletes according to the concrete requirements of each activity(36,37,38,39).
The objectives of this phase are to:
• Achieve the normalization of strength, resistance, neuromuscular control and power.
• Secure a gradual and controlled increase in anterior capsulolabral stress.
• Gradually restore activities of daily living, and occupational and leisure activities.
The following actions and exercises are to be avoided:
• Effort involving excessive stress of the anterior capsule.
• Specific sports training if full strength and joint balance are not achieved.
• Parallel bar dips.
• Bar and weight exercises starting from full flexion of the shoulders and which move the load to behind the head.
Early functional phase
Functional recovery starts in this phase. A gradual transition therefore should be carried out from the activities of the previous phase to those of the new phase - in all cases individualized according to the needs and tolerance of the patient. In this stage it is not yet advisable to introduce specific sports activity, but we can begin to train the usual sports manoeuvres with low loads. This phase usually extends from approximately week 12 to week 20.
The exercises that can begin include those involving full flexion of the shoulder with weight (military press exercise) and rowing exercises with the shoulders below 90°, progressing to above 90° conditioned to tolerance. Flexion exercises in the form of push-ups can also be started, without bending the elbows more than 90°.
Plyometric training can begin in this phase, and can be intensified as patient tolerance increases. This constitutes specific muscle training to gain strength and speed simultaneously, with repetitions under loading conditions and at growing speeds. In order to start these exercises, the patient must have reached strength 4+/5 in the complete scapular girdle, as well as full joint balance, and should be able to perform activities of daily living without pain(1,13). We normally begin with exercises based on elastic elements at low speeds, placing special emphasis on the precision and quality of the exercise before advancing in the number of repetitions (e.g., start with 3-5 series of 15-20 repetitions a week). The speed of the activities can be increased from week 16, provided they have previously been carried out with adequate control and no compensatory manoeuvres at low and moderate speed. This training is especially important for throwing athletes, who perform exercises at increasing speeds and loads in different spatial planes until finally seeking to reproduce the competition sports manoeuvre(13,40).
Late functional phase
In this stage we eliminate the movement restrictions of the indicated exercises. We can therefore start strength exercises in positions of maximum abduction and ER in open kinetic chain, though always on a progressive basis according to tolerance and with gradual load increments(41).
We should intensify training of the specific sports manoeuvre with progressively increasing loads until clinical normalization is reached. In throwing athletes, plyometric training should be taken to the last planned stages, seeking to reproduce the sports manoeuvre with the greatest speed possible. Once this has been achieved, the patient can return to competition sports activity.
Return to sports activity
The optimum time for returning to sports activity is a constant source of controversy. Most of the published protocols do not contemplate such a return before 6 months, though the period may vary according to the type of sports(13,32). Ialenti et al.(42), in a systematic review and meta-analysis of studies with level III-IV of evidence, found that patients return to competition contact sports activity an average of 6.1 months after anterior capsulolabral repair surgery, and that 71% reach competition levels similar to those before the operation. These findings have been corroborated by other authors, with no significant variations in the time to return to sports activity(43). However, after 6 months, approximately half of the athletes present function and strength levels below 90% versus the contralateral shoulder(44). It is therefore necessary to consider whether a longer time is needed before returning to sports activity. In this regard, a number of studies have analysed the results of protocols allowing a return to sports based on specific functional criteria referred to each type of sport, instead of using strict time criteria. Although the percentage of athletes that returned to competition activities at a satisfactory level was seen to be high, great variability was observed in relation to the moment of return(45,46).
Throwing athletes require a longer recovery period, since the fundamental sports manoeuvre in such cases can cause the original injury to recur. The incidence of return to sports activity in this subgroup of athletes is good following anterior capsulolabral repair, though the performance reached after the operation is not so good - since most patients describe a decrease in throwing speed, and relapse in terms of pain and instability is frequent(47). Thus, the different published studies and protocols agree on a longer duration of rehabilitation in these individuals, and no publication has been found contemplating a return to sports activity in less than 7 months(43,46,47).
Recommendations on the return to sports activity
• There is no concrete time limit from which an athlete can be allowed to return to his or her activity.
• The decision depends on the function achieved, the strength obtained and the capacity to perform the corresponding sports manoeuvre.
• Throwing athletes require longer recovery periods than non-throwing athletes.
Conclusions
The progression of rehabilitation following anterior capsulolabral repair surgery should be adapted to the tolerance of each individual patient. It is essential to divide the process into phases - each with clear objectives defining the interventions to be carried out. In the present study we propose three phases: in the first phase the aims are repair protection and adequate analgesia to allow closely controlled passive mobilization. The second phase seeks to complete restoration of the active range of motion, as well as correct the possible scapular dyskinesias. The third phase aims to recover muscle strength and reintroduce the daily or sports activities.
Figuras
Figure 1. Most important aspects during the protection phase.
Figure 2. A: active elbow flexion exercise; B: active elbow extension exercise; C: Codman pendulum exercise.
Figure 3. Isometric exercises of the deltoid muscle.
Figure 4. A: passive elevation exercise with bar; B: step-back passive elevation exercise with table.
Figure 5. A: passive external rotation exercise with bar; B: scapular retraction exercise.
Figure 6. A: pectoralis minor assisted stretch exercise; B: internal rotation assisted stretch; C: sleeper stretch.
Figure 7. A: anterior serratus exercise on all fours; B: anterior serratus exercise in standing position.
Figure 8. Measures destined to correct scapular dyskinesia following arthroscopic anterior capsulolabral repair.
Figure 9. A: low row strength exercise; B: lawnmower strength exercise.
Figure 10. Most important aspects during the active recovery phase.
Tablas
Table 1. Mobility objectives during the active recovery phase.

Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors state that they have no conflicts of interest.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved studies in humans or in animals.
Data confidentiality. The authors declare that the protocols of their centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Young Arthroscopy Group (Grupo Joven de Artroscopia [GJA])
This study has been coordinated and carried out within the context of the Young Arthroscopy Group (Grupo Joven de Artroscopia [GJA]) project of the Spanish Association of Arthroscopy (Asociación Española de Artroscopia [AEA]).
Acknowledgements
Thanks are due to Dr. Ángel Calvo Díaz and to Dr. Néstor Zurita Uroz for their supervision and critical review of the present study.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- <em>REACA</em>: school for authors
- Reconstruction of the medial patellofemoral ligament is effective in treating lateral patellofemoral instability, even in the presence of trochlear dysplasia. A review of 18 cases
- Results of the survey on the use of ultrasound among the members of the Spanish Association of Arthroscopy (Asociación Española de Artroscopia [AEA])
- Management of anterior glenohumeral instability without significant glenoid bone damage
- Rehabilitation following anterior capsulolabral arthroscopic Bankart repair: a guide for the young arthroscopist
- Diagnosis and management of injuries of the anterior cruciate ligament in skeletally immature patients. A narrative review
- Residual instability after reconstruction surgery of the anterior cruciate ligament. What are we missing?
- Posterolateral instability of the knee following osteochondral fracture including the femoral insertion of the popliteus tendon. A case report
- Meso-type long portion of the biceps: normal anatomical variant
- Instructions for authors (Apr. 2021)
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.