
Management of triceps surae muscle injuries in young adult and middle-aged athletes: a narrative literature review
Manejo de las lesiones musculares del tríceps sural en deportistas adultos jóvenes y de mediana edad: revisión narrativa de la literatura
Introduction
Injuries of the triceps surae muscle were first described in 1883 in tennis players - hence the term "tennis leg"(1). Such injuries can be classified as proposed by Dixon(2) and described in Table 1. Together with other injuries of the leg and of the Achilles tendon in professional football players, these lesions may account for up to 11% of all injuries suffered in the course of professional sports activities(3). In addition, it is common to observe triceps surae injuries in young adult and middle-aged athletes in sports such as tennis, basketball, running or football(1). Unfortunately, these injuries cause important pain, claudication, oedema, functional impotence and significant loss of sports performance(4). This is because the triceps surae is the muscle group in charge of propulsion and the absorption of forces in the lower extremity upon impacting on the floor(5). Thus, a correct and opportune diagnosis of injuries of the triceps surae muscle in young adult and middle-aged athletes is essential in order to adopt management strategies allowing efficient and adequate recovery of the athlete(4).
reacae.29175.fs2002013en-table1.png
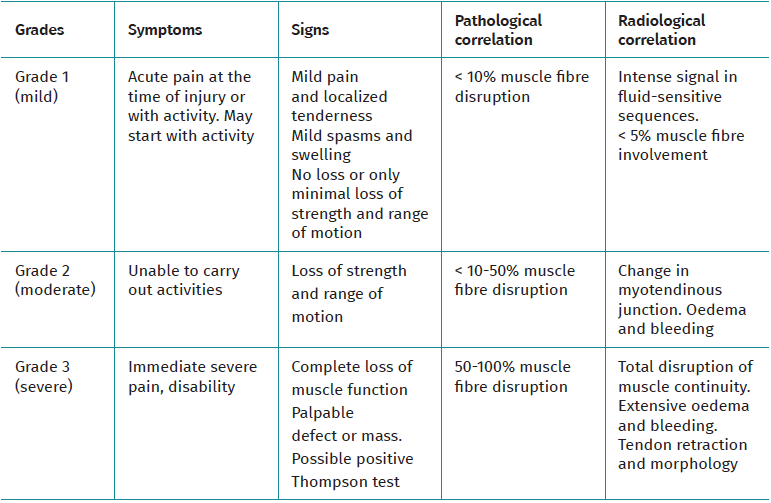
Table 1. Classification of triceps surae injuries into three grades
The triceps surae is composed of the medial and lateral gastrocnemius, soleus and plantaris muscles. Their aponeuroses join at distal level to give rise to the Achilles tendon, which inserts in the calcaneal tuberosity, thereby defining the muscle group as a plantar flexor when its muscle action is concentric(6). As a result, triceps surae injuries often arise in maximum extension of the knee with a dorsiflexion of the ankle, since this distends the triceps surae and all the anatomical elements located in the posterior compartment of the leg(7,8,9). Both an increase in tension of the elastic elements and high velocities predispose to plastic deformation of the elastic structures of the triceps surae, generating ruptures, especially during the eccentric phase of muscle contraction, characterized by proximal muscle traction in addition to distal traction through over-stretching(6). Since the triceps surae crosses more than one joint and is largely composed of type 2 or fast-twitch fibres, high-velocity eccentric contractions are considered to pose a high risk of causing muscle tearing(2). In addition, other factors such as muscle fatigue, altered interarticular coordination (knee-ankle) or deteriorated vascularisation can increase the risk of triceps surae tearing(1).
Although injuries of the triceps surae muscle are frequent in athletes and the mechanism of injury is clear(2), the anatomical differential diagnosis of injuries of the gastrocnemius, soleus and plantaris muscles, as well as their magnitude, may prove difficult(10). The complex anatomy of this muscle group complicates the diagnosis, resulting in inadequate therapeutic management that can adversely affect the performance of the athlete(10). For this reason, it is necessary to improve identification of the anatomical location of the injury and to establish its magnitude. A careful clinical history and physical examination are thus required(9). In addition, the use of complementary techniques such as magnetic resonance imaging (MRI) and ultrasonography can improve the diagnosis of the muscle lesion(11,12). Depending on the magnitude of the injury, the suggested treatment may be either conservative or surgical(12). In addition, it is advisable to use biological coadjuvants such as platelet rich plasma (PRP) to shorten the muscle injury recovery period and improve the healing process(13,14). However, there is currently no scientific evidence consistently supporting their use to relieve the pain and improve function and return to sports activity following a muscle injury(14). This is probably because these factors are more associated to joint function(11).
The present study offers a narrative literature review of the management strategies (clinical history, clinical examination, imaging tests and treatment) in the triceps surae muscle injuries referred to above.
Methods
Study design
This narrative literature review was made by 5 independent experts between the years 2019 and 2020, with the aim of answering the following question: what are the suggested strategies for the management of triceps surae muscle injuries?
Inclusion and exclusion criteria
The inclusion criteria were: scientific articles (cohorts, cross-sectional studies, clinical trials, narrative reviews, systematic reviews and meta-analyses) addressing the clinical history, clinical examination, classification and treatment of triceps surae muscle tears among individuals involved in physical activity and/or sports between 18-45 years of age. The articles were required to be written in Spanish or English, and to be published in journals indexed by PubMed (https://pubmed.ncbi.nlm.nih.gov/). In addition, full inclusion consensus among the authors was required, and both the title and the abstract of the publications had to be directly related to the research question. The exclusion criteria were: articles including individuals with comorbidities, collagen diseases, malnutrition, traumatic injuries other than tearing of the triceps surae muscle, and any described malformations of the study population. Clinical cases studies, case series, impossibility of access to the full-text articles, and publications not subjected to peer review were also excluded.
Results
Clinical history and clinical examination
In relation to the clinical history, clarity regarding the etiopathogenesis, clinical manifestations and epidemiology, and a structured patient interview, are essential. In addition, a guided investigation of the mechanism of injury is crucial for starting effective management of triceps surae muscle injuries. The prodromal symptoms of the gastrocnemius muscle facilitate the approach to the diagnostic hypothesis.. Approximately 20% of the patients may recall prodromal discomfort, with possible dull pain sensation in the affected leg(15). In the case of injury known as tennis leg, the patient typically describes a sudden uncomfortable blow sensation in the posterior region of the leg - in some cases accompanied by an audible click like the snapping of a branch(16). Likewise, at the time of the injury the patient might feel no pain, though the latter subsequently develops in the posteromedial zone of the leg and may become sufficiently intense to restrict walking capacity(17).
On the other hand, the physical examination allows us to establish the location and severity of the injury. In order to establish a differential diagnostic hypothesis of the possible tearing of the triceps surae muscle, the use of provocation tests and pain relieving manoeuvres based on palpation, strength tests and elongation of the medial and lateral gastrocnemius and soleus muscles are essential for locating the possible lesion(18). In addition, the literature suggests that differentiating between damage to the gastrocnemius and the soleus muscle is clinically important in order to guide treatment and determine the prognosis of these injuries(19).
The examiner firstly should isolate muscle activation, varying the degree of flexion of the knee. For example, with the knee in maximum flexion, the soleus becomes the first force generator in plantar flexion. In contrast, with the knee in maximum extension, the gastrocnemius makes the greatest contribution to plantar flexion(2). This behaviour is explained by the mechanical differences between the gastrocnemius and the soleus, as these muscles are inserted proximally and distally to the knee, respectively. Therefore, in order to perform a soleus muscle provocation test, plantar flexion with flexion of the knee is required, while a gastrocnemius provocation test requires plantar flexion with extension of the knee. Furthermore, it is advisable to palpate the posterior region of the leg along the length of the muscle and its aponeurosis(18). At this point it is necessary to assess the pain response to palpation, the level of inflammation, thickening or defects, and masses. The topology of the pain response is important in the physical examination, because tearing of the gastrocnemius muscle typically manifests with pain at the medial surface or myotendinous junction, while pain in the case of tearing of the soleus is generally located lateral(20).
The possible findings of the physical examination include pain at the site of the tear, ecchymosis(19) or a subcutaneous gap. The latter sign implies tissue retraction and indicates increased severity of the lesion(19). In this respect, the patient may report intense pain during passive elongation of the triceps surae or during plantar flexion against resistance(18).
Some additional tests may be used in the differential evaluation of triceps surae muscle tears with the aim of provoking dysfunction of the propulsion and plantar flexor buffering mechanism. This includes the Thompson test or squeeze test, performed in supine decubitus with compression of the plantar flexor mechanism; circumferential measurements of the leg to quantify asymmetry, performed with the patient in the standing position in the most prominent zone of the leg; and the evaluation of functional movements(21,22). These movements include monopedal raising of the heel (which can be performed in the standing position, with mild assistance from the upper extremity); bipedal raising of the heel (performed in the same modality as the previous test); closed chain dorsiflexion (performed in the standing position; with the sole of the foot fully supported, the weight of the body is carried forward to generate tension in the posterior muscles of the leg); jumping on one leg (performed in the standing position, with vertical impulsion); walking and running (preferably using a biomechanical unit)(23). Lastly, it must be taken into account that concomitant injuries of the soleus and gastrocnemius may complicate the differential diagnosis, due to the combination of clinical symptoms and signs. This combination has been described in up to 17% in all radiological studies(24), i.e., approximately one out of every 6 patients may present such combined manifestations.
Imaging tests
The differential diagnosis of triceps surae muscle lesions is broad and includes rupture of the Achilles tendon, vascular impingements, chronic exercise-induced compartment syndrome, plantaris injury and deep vein thrombosis (DVT) - the latter being a condition requiring adequate identification and treatment(25).
Ultrasound is the initial imaging technique of choice, due to its rapid accessibility, low cost and the absence of radiation(26,27,28), as reflected in Figure 1. Some of the features to be evaluated by ultrasound are the size of rupture, whether rupture is total or partial, and the presence of haematoma and/or fluid collections between the gastrocnemius and the soleus.
reacae.29175.fs2002013en-figure1.png
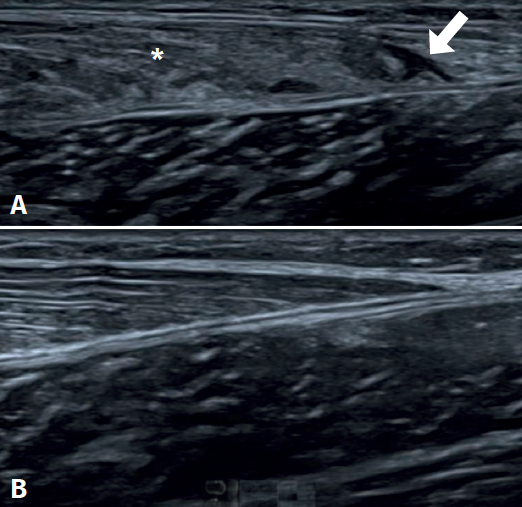
Figure 1. Ultrasound study of triceps surae injuries. A: fibrillar damage of the distal myotendinous junction of the medial gastrocnemius muscle, showing the hypoechogenic fibrillar defect (arrow) associated to loss of the usual fibrillar pattern and oedema of the adjacent muscle fibres (asterisk); B: distal myotendinous junction of the medial gastrocnemius in a normal triceps surae muscle.
The most frequent ultrasound finding in triceps surae muscle injuries is a hypoechogenic zone at the distal myotendinous junction of the medial gastrocnemius muscle(29). The latter appears as a serohematic content between the muscle fibres and the myofascial plane, associated to an increase in echogenicity of the adjacent musculature as a manifestation of oedema and hyperaemia in the colour Doppler study(9), as can be seen in Figure 1. Delgado et al., in 141 patients clinically diagnosed with tennis leg, found that 67% of the patients presented partial rupture of the medial gastrocnemius, 1.4% presented associated plantaris tendon rupture, and 21% presented an intermuscular fluid collection between the medial gastrocnemius and the soleus muscle - thus affording an improved perspective of the possible differential diagnosis(30). On the other hand, involvement of the lateral gastrocnemius is much less common (up to 14% of the cases)(31). Ultrasound also plays a role in the lesions follow-up. In a normal evolutive scenario, we can observe gradual reduction of the oedema, resolution of the fibrillar defect and reabsorption of the fluid collections(32). It is also common to observe signs of organization of the haematoma between the gastrocnemius and the soleus, evolving as a fusiform fibrous scar without inflammatory elements, as can be seen in Figure 2.
reacae.29175.fs2002013en-figure2.png
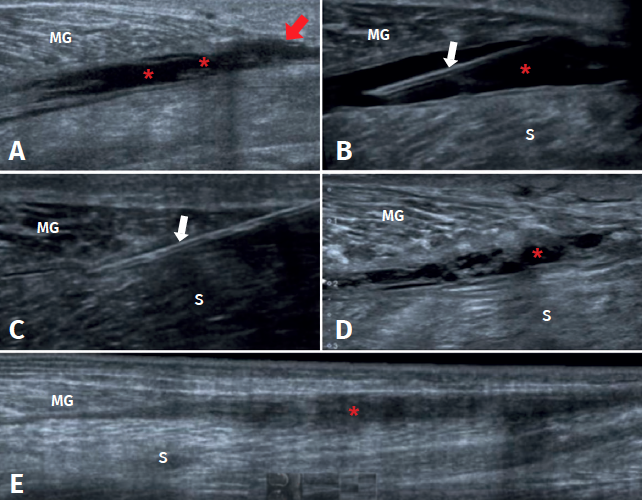
Figure 2. Evolution of a medial gastrocnemius fibrillar tear. A: ultrasound view of an acute tear of the distal myotendinous junction of the medial gastrocnemius (MG) (red arrow), associated to haematoma in the aponeurotic plane adjacent to the soleus (S) (asterisks); B: needle positioning before aspiration (white arrows) of the haematoma under ultrasound guidance; C: needle aspiration (white arrows) of the haematoma under ultrasound guidance, extraction of 70 cc; D: control after 10 days, haematoma relapse, of smaller size, with septa and signs of organization; E: control after 31 days, showing organization of the haematoma, evolving towards a fibrous scar cord, without signs of inflammation. Complete healing of the tear (red arrow).
Ultrasound allows us to distinguish between muscle injury and DVT. Up to 10% of all suspected triceps surae injuries in fact correspond to DVT, which requires specific treatment and may give rise to life-threatening complications(25). It is therefore important to maintain a high degree of suspicion of such lesions(25,30).
reacae.29175.fs2002013en-figure3.png
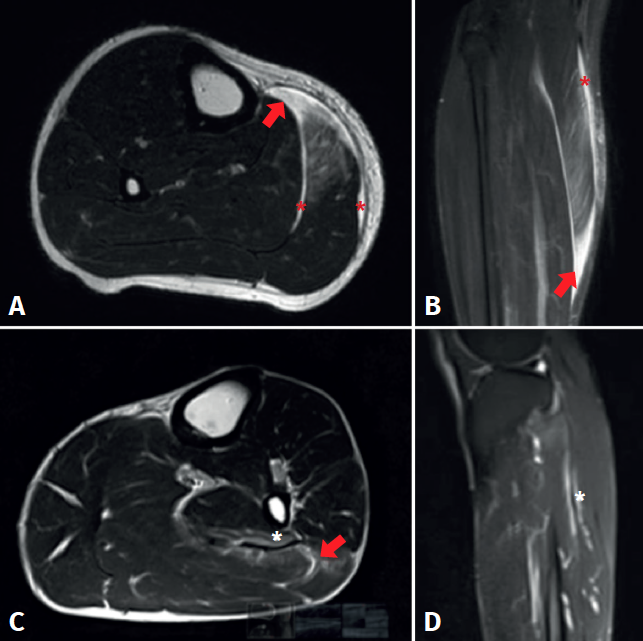
Figure 3. Magnetic resonance imaging study of triceps surae injuries. A: T2 axial sequence; B: coronal STIR sequence showing a fibrillar defect (red arrow) in the myotendinous junction of the medial gastrocnemius muscle, associated to a haematic collection in the peri-aponeurotic plane (red asterisks); C: T2 axial sequence; D: T2 FS sequence showing a fibrillar defect of the soleus muscle in the lateral proximal myotendinous junction (red arrow) associated to oedema of the adjacent muscle fibres (white asterisks).
Magnetic resonance imaging (MRI) facilitates the differential diagnosis, due to the greater anatomical details it provides. The signs that can be identified by MRI include oedema, muscle fibre rupture or discontinuities, muscle retraction and the presence of haematomas, as seen in Figure 3. With the use of MRI, muscle lesions are easily identified and located - the percentage frequency of damage to the medial gastrocnemius and the soleus being similar(33). In contrast, ultrasound is less capable in diagnosing these muscle injuries(9). In this context, 5 important soleus muscle injury sites have been described: at the medial proximal myotendinous junction (25.5%), the lateral proximal region (12.7%), the central and distal portion of the Achilles tendon (18.2%), and in the anterior and posterior myofascial plane (43.6%)(34), as can be seen in Figure 3. Balius et al. compared the capacity of ultrasound to diagnose soleus injuries versus MRI. The authors found that ultrasound was only able to detect 27.2% of the cases - the best detection performance corresponding to lesions in the posterior myofascial plane(34). Therefore, in cases with a strong clinical suspicion of tearing of the soleus muscle, and in the presence of normal ultrasound findings, MRI should be used in the differential diagnosis of the disorder.
Treatment
An early objective in the management of the acute phase of triceps surae injuries is to limit bleeding and pain, and prevent complications(35,36).
Muscle resting is advised in the first 3-5 days, with the limitation of muscle elongation and contraction, the application of cryotherapy and compression, raising of the leg, and analgesia(32,37,38,39). The use of compression bandages, a heel wedge or lift, and walking with the help of walking sticks are useful during this phase. The use of nonsteroidal anti-inflammatory drugs (NSAIDs) should be limited to the first 24-72 hours due to the increased bleeding associated with their anti-platelet action. In contrast to NSAIDs, the prescription of COX-2 inhibitors represents a therapeutic alternative during this period, since they have no anti-platelet aggregation effects(36). Paracetamol, opiate analgesics and electroanalgesia can also be used for pain control(37). As an absolute contraindication at the lesion site or adjacent locations, moist heat and massage in the early healing phase is not advised, due to the increased bleeding risk(12). In this stage, special care is required regarding compartment syndrome which, though infrequent, can complicate the course of acute muscle tearing. It is therefore relevant to instruct the patient on the symptoms of this complication and ensure that they are promptly reported(37). If the symptoms persist or do not improve as expected with the acute treatment provided, re-examination and further imaging tests are indicated in order to evaluate the complications and redirect the treatment strategy.
In the subacute phase (7-10 days), fluid collections can be aspirated under ultrasound guidance to improve the rehabilitation process(32). Succinctly, aspiration preferably should be made in the subacute phase, and proves more effective if fluid is obtained (versus pure haematoma) and total drainage of the serohaematic collection is achieved(40). Special care to avoid iatrogenic neurovascular problems is required(40). On the other hand, it is essential to restrict the technique in the presence of active bleeding, coagulopathy or a lack of skill in handling the needle and ultrasound system(40). Figure 2 details the course of a medial gastrocnemius fibrillar tear and total drainage of the fluid collection in a patient prior to rehabilitation.
The start of physical rehabilitation is suggested in the same aforementioned subacute phase of triceps surae injuries(28). In this stage, the objectives of treatment are: to favour the healing process, reinforce the scar, condition and strengthen the affected muscles, and ensure early identification of alterations in muscle contraction(37). Ten days after the injury, the scar that has developed is expected to afford an increase in tension resistance allowing progress towards isometric strengthening exercises, which always should precede concentric and eccentric exercises(28,37). In this stage, physiotherapeutic methods such as moist heat, deep warmth and the therapeutic management of soft tissues are relatively permissible, provided that they do not give rise to inflammatory processes(37). Passive elongation of the injured muscle will help to deform the maturating intermuscular scar and will serve as a stimulus (deformation of membrane proteins) for collagen synthesis and the rearrangement of fibres in the directions of the muscle work action lines(41,42). It is crucial to achieve this before the muscle strengthening phase. Progression towards dynamic training should take place in the measure that each exercise can be made without pain(12,20). In relation to the concentric and eccentric strengthening exercises, it is advisable to start them only if moderate isometric strengthening can be carried out without pain(28,37). Subsequently, functional rehabilitation should be implemented considering neuromuscular aspects and multitask movements to improve strength, resistance and motor skills(37). Afterwards, during the period of the patient return to sports activities, plyometric and ballistic training should be prescribed in order to prevent injury relapse(37). As a final stage, muscle function should be subjected to re-evaluation to determine biomechanical performance, complemented by clinical scores to quantify and assess the current condition of the muscle injury. It is particularly here where a guided assessment is required of a possible lack of eccentric strength, eccentric control and neuromuscular alterations.
It is relevant to consider the biomechanics of the damaged muscles in rehabilitation. While it is advisable to train the soleus muscle as a muscle with greater tolerance to fatigue, training of the gastrocnemius should focus on muscle power. Another relevant aspect is to view rehabilitation as a process that can vary temporarily according to the lesion grade (Table 1). In this regard, grade 1 injuries have a good prognosis and evolve satisfactorily with the previously described tissue repair timelines, while grade 3 injuries may have a poorer functional prognosis, with a risk of relapse and overload. A poorer lesion prognosis is also to be expected particularly if the myotendinous junction or tendon are affected. Unfortunately, an increased loss of muscle fibres, as in grade 3 injuries, may affect the neuromuscular activity and muscle synergies that require a longer rehabilitation period, with a need for muscle re-education that is not seen in the other injury grades.
As biological coadjuvants to healing, PRP is often used in muscle injuries because it has been suggested to improve healing(28) and shorten the time to recovery of the lesion(13,14). However, the mechanisms whereby PRP produces its effects in some patients are not fully clear. In a systematic review including 23 studies (15 in vivo, 6 in vitro, 2 in vivo/in vitro), only one reported the complete PRP cytological profile (platelets and red and white cell counts). 5 in vitro studies reported cell proliferation, f4 reported increased genic expression, 3 described greater muscle regeneration, and 7 reported improved histological quality of the muscle tissue(43). The basic science literature on the use of PRP in muscle diseases shows PRP treatment to afford a number of potentially beneficial effects in healing versus the controls(43). However, further research is needed to define the optimum PRP cytology, dosage, timing and delivery methods in muscle diseases(13).
There are special situations in which surgical treatment may prove necessary. This is the case of rupture of the medial head of the gastrocnemius, which typically occurs when the muscle has been over-stretched by ankle dorsiflexion with the knee extended - causing total or subtotal damage to the myotendinous junction(37). Repair with reinsertion using sutures is advised in this scenario, in view of the poorer prognosis. The typical presentation corresponds to a middle-aged person practising sports and who experiences acute pain in the middle portion of the posterior surface of the leg, associated to a clicking effect. Evaluation of this lesion using MRI is suggested. Surgical indication should focus on myotendinous injuries of the gastrocnemius or soleus muscle occurring in young individuals who are active in sports, with a view to ensuring early anatomical restoration and improved rehabilitation - thereby making it possible for the patient to continue with his or her sports activities. However, some authors advocate surgery in cases of complete muscle rupture, corresponding to grade 3 injuries (Table 1), and for patients with chronic pain (4-6 months) presenting evidence of triceps surae contracture, in order to perform a release procedure(44). Finally, large intramuscular haematomas may impede clinical improvement and are also an indication for surgery(44).
Lastly, it always must be considered that a torpid course may be indicative of the presence of myositis ossificans. Physical examination therefore should be guided to assess rigid densities in the scar tissue, with plain radiographs serving to establish the diagnosis(37).
Conclusions
The clinical management of triceps surae muscle injuries in young adult and middle-aged athletes should be conducted on a systematic basis, taking into account the clinical history, the physical examination and imaging tests that may contribute to a better differential diagnosis and choice of treatment. Special attention must focus on the possible development of DVT, myositis ossificans, compartment syndrome and relapses, the application of biomechanical tests, and mistaken early patient discharge. Most studies indicate that gastrocnemius muscle tears have a good prognosis provided that adequate management is ensured. However, neither early discharge nor excessively conservative treatment favour an adequate return to physical or sports activity. Amongst the different triceps surae injuries, those of the soleus are initially underdiagnosed, and the diagnosis is often only established in subacute stages. Lastly, further quality research is needed to define the clinical effects of coadjuvant biological therapies such as PRP and the surgical interventions of triceps surae muscle injuries.
Tablas
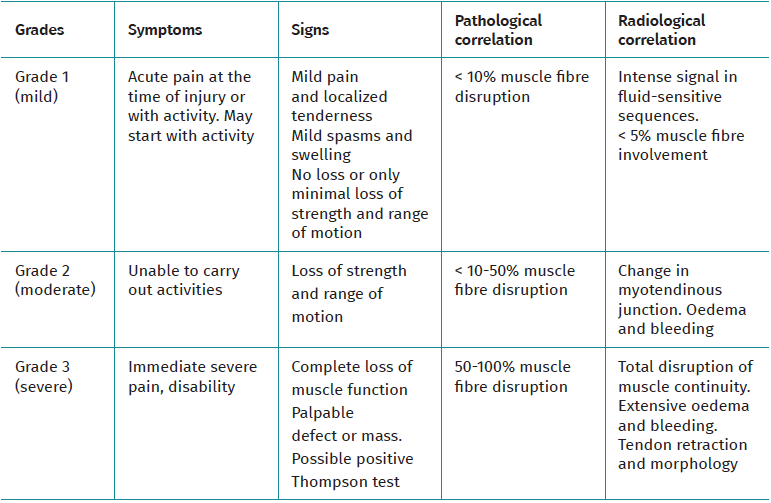
Table 1. Classification of triceps surae injuries into three grades
Figuras
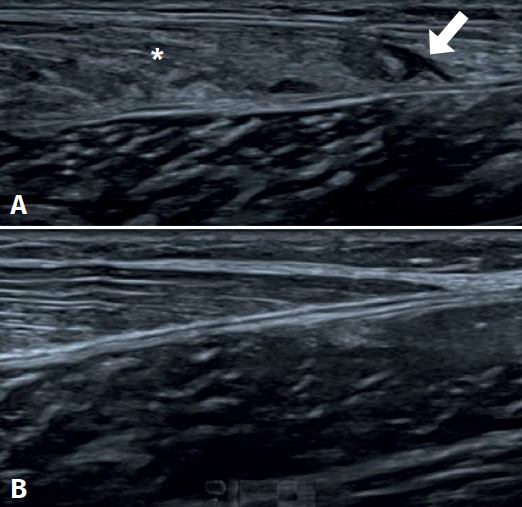
Figure 1. Ultrasound study of triceps surae injuries. A: fibrillar damage of the distal myotendinous junction of the medial gastrocnemius muscle, showing the hypoechogenic fibrillar defect (arrow) associated to loss of the usual fibrillar pattern and oedema of the adjacent muscle fibres (asterisk); B: distal myotendinous junction of the medial gastrocnemius in a normal triceps surae muscle.
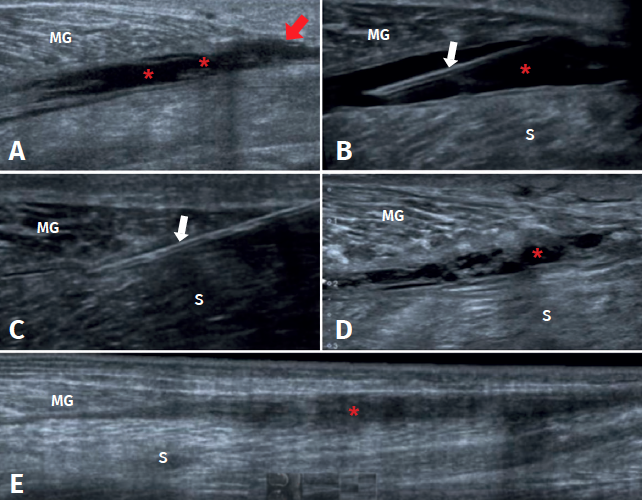
Figure 2. Evolution of a medial gastrocnemius fibrillar tear. A: ultrasound view of an acute tear of the distal myotendinous junction of the medial gastrocnemius (MG) (red arrow), associated to haematoma in the aponeurotic plane adjacent to the soleus (S) (asterisks); B: needle positioning before aspiration (white arrows) of the haematoma under ultrasound guidance; C: needle aspiration (white arrows) of the haematoma under ultrasound guidance, extraction of 70 cc; D: control after 10 days, haematoma relapse, of smaller size, with septa and signs of organization; E: control after 31 days, showing organization of the haematoma, evolving towards a fibrous scar cord, without signs of inflammation. Complete healing of the tear (red arrow).
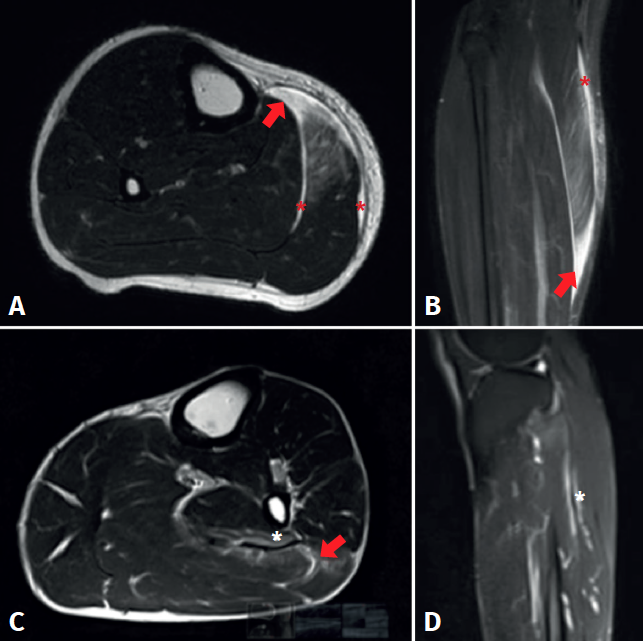
Figure 3. Magnetic resonance imaging study of triceps surae injuries. A: T2 axial sequence; B: coronal STIR sequence showing a fibrillar defect (red arrow) in the myotendinous junction of the medial gastrocnemius muscle, associated to a haematic collection in the peri-aponeurotic plane (red asterisks); C: T2 axial sequence; D: T2 FS sequence showing a fibrillar defect of the soleus muscle in the lateral proximal myotendinous junction (red arrow) associated to oedema of the adjacent muscle fibres (white asterisks).

Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors state that they have no conflicts of interest.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- Tendon injury: from eternally forgotten to trendy disease
- Physiology and mechanobiology of tendon and muscle tissue
- Patellar tendinopathy: diagnosis by ultrasound and magnetic resonance imaging. Conservative and surgical management alternatives
- Pathophysiology, diagnosis and treatment of Achilles tendinopathy
- Supraspinatus tendinopathy: diagnosis by ultrasound and magnetic resonance imaging. Conservative and surgical management alternatives
- Results of arthroscopic gluteus medius tendon repair in patients with trochanteric pain syndrome. Case series
- Update on the diagnosis and treatment of quadriceps muscle injuries
- Management of triceps surae muscle injuries in young adult and middle-aged athletes: a narrative literature review
- Insertional tendinopathy of the Achilles tendon. Treatment from start to finish
- Inverted cyclops
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.