
Fully arthroscopic osteosynthesis with button placement in acute anterior glenoid fracture: a case report
Osteosíntesis completamente artroscópica con botón de fractura aguda de glenoides anterior: reporte de caso
Introduction
Traumatic glenohumeral dislocation can be accompanied by fractures of the anterior glenoid margin or labrum. These joint injuries must be adequately managed in order to avoid complications over the middle to long term, such as recurrent instability or early osteoarthrosis(1). In the case of angled fractures or with displacement > 5 mm, defective joining of the fragment can result in unsatisfactory clinical outcomes, with surgical treatment being advised in such situations(2). Different approaches are available for treating these injuries, which constitute a challenge due to their anatomical location close to critical neurovascular structures. In addition, the open approach may compromise the tendon of the subscapularis muscle, causing damage or insufficiency of the latter. For this reason, arthroscopic support constitutes a tool for reducing soft tissue morbidity, and offers additional advantages such as more precise assessment of the quality of reduction of the fragment and treatment of the concomitant joint disease in the same surgical step(3). On the other hand, these fractures traditionally have been fixed with screws, which can cause neurological damage or cause discomfort due to their prominent profile, with the need for surgical removal once the fracture has become consolidated. With the aim of reducing these inconveniences, flexible fixation techniques have been proposed, such as arthroscopic double button fixation systems, which have shown good results in fixing bone grafts in bone block procedures(4,5,6).
We present the case of a woman with fracture of the anterior glenoid labrum subjected to fully arthroscopic surgery with this type of fixation.
Case description
A 55-year-old woman with hypothyroidism as the only medical history of interest was admitted due to right anterior glenohumeral dislocation following a fall. The computed axial tomography (CAT) scan with three-dimensional (3D) reconstruction in en-face sagittal view of the glenoid cavity confirmed an acute glenoid fracture affecting 25% of the joint surface as measured with the "perfect circle" technique using the linear method to determine percentage bone loss(7,8). Measurement moreover found the displacement of the fragment to be 9.5 mm (Figure 1). Taking into account the size of the fragment and its displacement, arthroscopic surgery was decided for reduction and fixation using the button system.
reacae.30380.fs2307021en-figure1.png
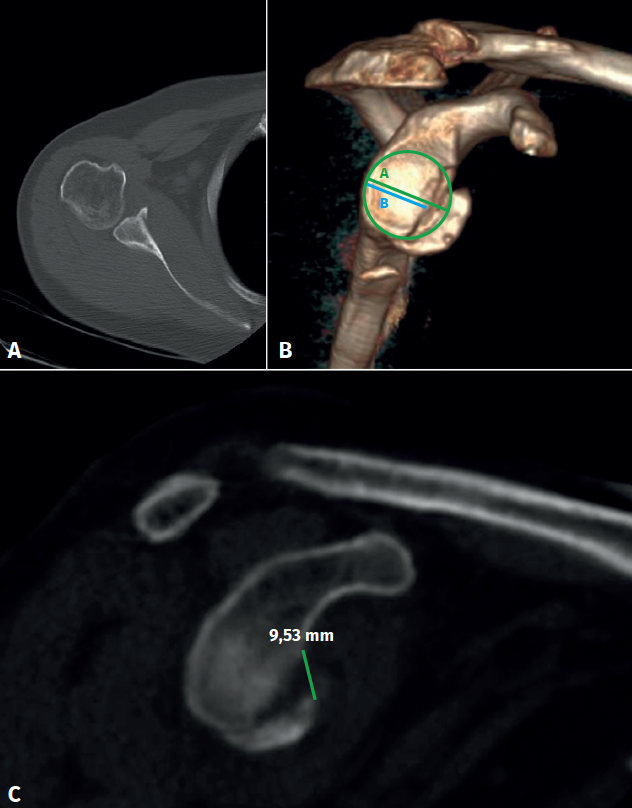
Figure 1. Presurgical images of the lesion. A: computed tomography view (axial section) showing the displaced fracture of the anterior glenoid labrum; B: three-dimensional reconstruction confirming displacement and a fracture fragment size corresponding to 25% of the glenoid surface, using the perfect circle method with linear calculation; C: computed tomography view (sagittal section) of the glenoid cavity, confirming displacement of the fragment (9.5 mm).
Surgical procedure
Under general anesthesia and peripheral interscalene block, the patient was positioned in left lateral decubitus. We initially used three main portals: a standard posterior portal, an anteroinferior portal over the upper margin of the subscapularis, and an anterosuperior portal at the level of the rotator interval. An accessory posterior portal was later required, parallel to the glenoid surface, created with the outside-in technique. A posterior arthroscopic approach was made, using the anterosuperior and anteroinferior arthroscopy portals with the outside-in technique. An 8.5-mm cannula was placed in the anteroinferior portal, and a 7.0-mm cannula was placed in the anterosuperior portal. The initial diagnostic arthroscopic exploration confirmed an anteroinferior glenoid fracture affecting 25% of the joint surface, in addition to anterosuperior capsule-ligament damage with intact lower ligaments, with a 10% non-engaging Hill-Sachs lesion.
Initially, with the camera in the anterosuperior portal, an elevator was used from the anterosuperior portal to separate the fragment from the anterior capsule and glenoid cavity. At this point it is essential not to exceed release in the lower region, since the fulcrum of the intact lower capsule is fundamental for anatomically positioning the fragment through upper traction of the latter from the anterosuperior capsular region. The fragment was reduced by exerting traction with arthroscopic retriever forceps from the upper capsule to prevent it from fracturing. Debridement of the fracture site was carried out. Reduction and fixation were made using a glenoid guide with hook. It is essential for this guide to be positioned fully parallel to the glenoid surface. If this is not done, the tunnels for correct button placement cannot be made, and anatomical reduction will not be possible. At this point, the previously mentioned accessory portal was prepared with the inside-out technique, checking its position with a needle. The guide was advanced using the fluted probe to extend beyond the posterior soft tissues. The guide hook was positioned at the upper part of the fragment. This allowed us to maintain reduction of the fragment for fixation, and the accompanying locking system allowed correct orientation of the orifices of the button system (Figure 2).
reacae.30380.fs2307021en-figure2.png
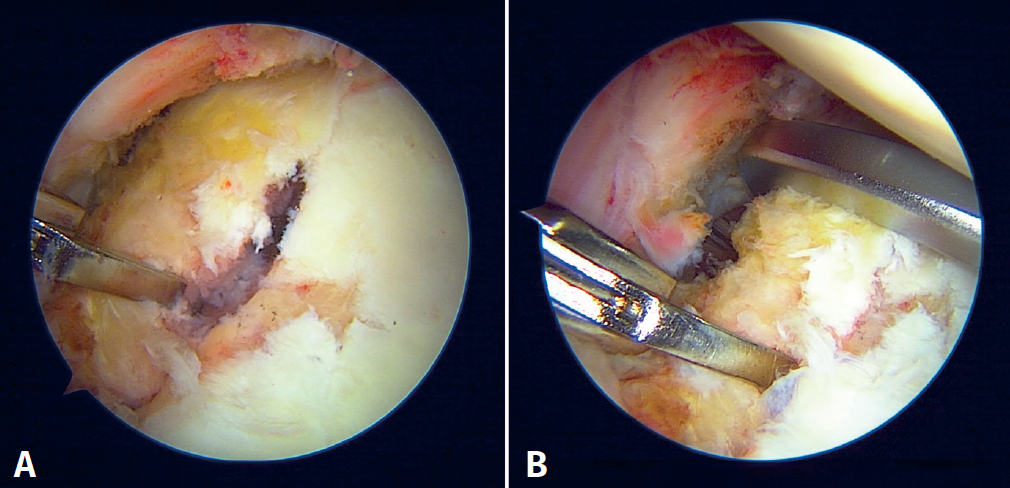
Figure 2. Initial findings of right shoulder arthroscopy with the patient in left lateral decubitus, with visualization from the anterosuperior portal. A: osteochondral fracture fragment of the anterior glenoid labrum; B: reduction with glenoid hook guide from the posterior portal.
Then, a guide orifice was drilled in the glenoid joint margin above the fracture site to position a knotless anchoring used for anterosuperior capsulolabral repair after osteosynthesis. It is important to perform such drilling before positioning the button system, in order to avoid damage to the latter during final capsular plication. Through the posterior portal we then positioned a Wissinger rod to deflect the capsule from posterior to anterior before drilling of the button system. This separation protects the axillary nerve if the drill inadvertently traverses the capsule. Using a guide with hook, a lower 2.8-mm orifice was drilled, parallel to the glenoid surface, through which a flexible transporter loop was advanced to position the button system for osteosynthesis (Figure 3). In this case, fixation with a single button proved sufficient and stable, since the lower glenohumeral ligaments were intact. At the level of the orifice, traction was exerted from anterior to posterior, sliding the double loop button system until it contacted with the fragment in the anterior region. At this point it is advisable to use an arthroscopic probe from the anterosuperior portal to correctly position the anterior button.
reacae.30380.fs2307021en-figure3.png
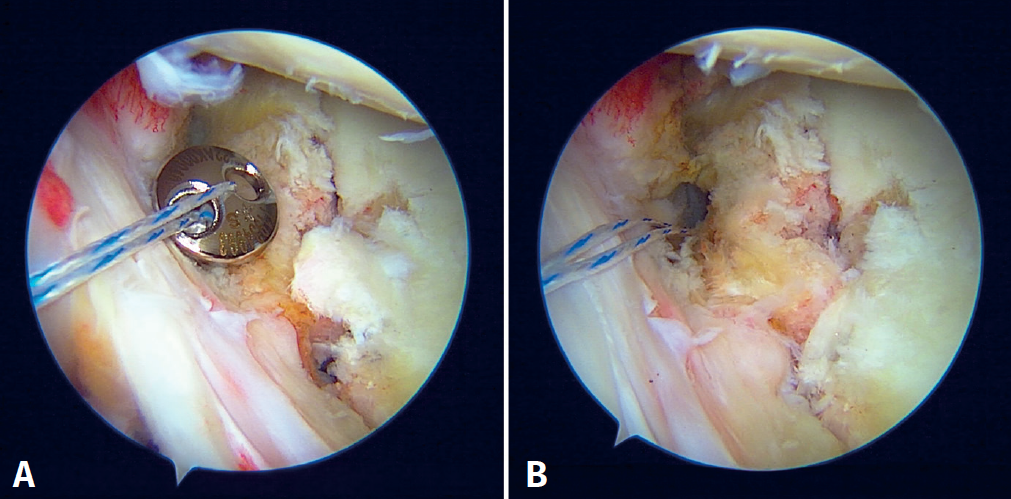
Figure 3. Shoulder arthroscopy images with the patient in lateral decubitus. A: fracture fragment with fixation using the arthroscopic button system; B: final anatomical reduction of the fragment.
Lastly, we positioned the posterior button, sliding it with a Nice knot. The sutures of the system were knotted and reduction was visually confirmed via arthroscopy, with compression using the mechanical tensor to 100 N in four cycles. Three safety knots were applied over the knot, and the sutures of the system were cut. Subsequently, capsulolabral repair was carried out with an arthroscopic band fixed at the anchoring without knots in the previously drilled orifice(9). The key points and potential complications are described in Table 1.
reacae.30380.fs2307021en-table1.png
Table 1. Tips and possible complications of the technique
After the procedure, the patient shoulder was immobilized in neutral position for four weeks, starting physical therapy three weeks after the operation, with gradual passive and then active assisted mobility after 6 weeks. Six months after surgery, the patient achieved active flexion 145º, external rotation 30º, internal T12, without pain, and was able to return to her work and physical activity. The American Shoulder and Elbow Surgeons (ASES) score was 87(10), and assessment of her shoulder with the Single Assessment Numeric Evaluation (SANE)(11) was 87%. The 3D reconstruction confirmed adequate fracture consolidation, without steps or gaps in the glenoid cavity (Figure 4).
reacae.30380.fs2307021en-figure4.png
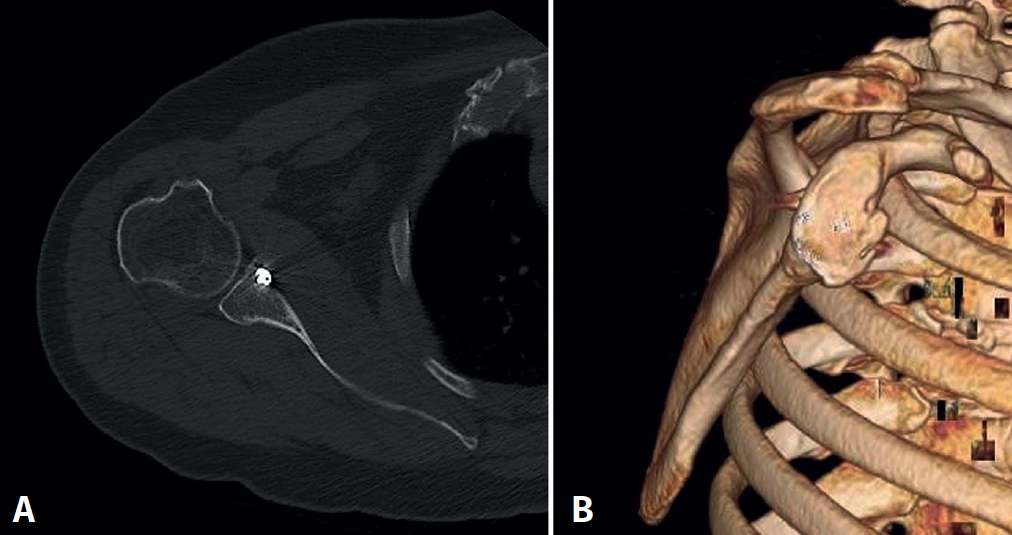
Figure 4. Computed axial tomography view 6 months after the procedure. A: sagittal view with the fracture consolidated and stabilized with the arthroscopic button; B: three-dimensional reconstruction.
Discussion
The present study describes a fully arthroscopic technique for the treatment of fractures of the anterior glenoid labrum using a button system. This is a flexible method, and when stabilized with a tensioning system, it affords adequate consolidation, avoiding the potential complications resulting from the use of screws and surgical approaches that involve greater morbidity.
Fractures of the anterior glenoid labrum are associated to glenohumeral dislocation in up to 21% of the cases(12), and although this is a joint fracture posing a potential risk of post-traumatic osteoarthrosis or joint instability, its treatment remains subject to controversy. In a study with a follow-up period of 5.6 years, Konninghausen reported that patients presenting fractures with displacement > 5 mm have poorer clinical outcomes and greater progression towards osteoarthrosis(2). In turn, Wieser presented results of the nonsurgical treatment of displaced glenoid fractures (mean displacement 8 mm) followed-up on over 9 years, with clinically satisfactory outcomes(13). However, one of four patients (25%) developed post-traumatic osteoarthrosis. Köningshausen et al., in a group of 36 patients followed-up on for 4.4 years with fragments corresponding to 21% of the glenoid surface on average, reported that although the results were mostly satisfactory, up to 30.5% of the patients developed osteoarthrosis at the end of follow-up, and the larger fragments tended to lead to poorer clinical outcomes on the functional scales(14). In contrast, Anavian et al., in a group of 33 patients with fractures presenting displacement > 4 mm and subjected to surgical treatment with a minimum follow-up of 27 months, reported satisfactory clinical outcomes as assessed with the Disability of Arm, Shoulder and Hand (DASH) scale and the SF-36, as well as in terms of mobility. Likewise, 90% of the patients were able to return to work, and consolidation of the fracture was confirmed in all cases(15).
The fixation of these fractures is technically demanding due to both the approach to the lesion and the possible complications associated to fixation. The open approach may cause morbidity and damage to the subscapularis. Initially, the fully arthroscopic techniques such as those described by Sugaya and Porcellini used fixation with bone anchorings in bony Bankart fragments corresponding to less than 25% of the glenoid surface, but these prove insufficient in larger fragments(16,17). In this technique two anchorings are used in the glenoid labrum and the upper and lower region of the fracture, knotting with the sutures of the anchorings of the capsulolabral region at the extremities of the fragment. Another method is the double-row, double-pulley technique described by Ganokroj(18). In this case an additional anchoring is used in the medial region at the glenoid chondral margin to secure fixation at two points and direct reduction with multiple knots around the fragment. Fernández et al. found that both this method and the double-row techniques for lesions corresponding to less than 15% of the glenoid surface afford satisfactory results without dislocation relapse or other complications over 28 months of follow-up(19). There have also been descriptions of osteosynthesis techniques assisted by arthroscopy for fixation with screws. However, the use of screws may cause damage to the brachial plexus or subscapularis, migration of the material and associated discomforts, making extraction necessary. Tauber et al., in a series of 10 patients with glenoid fractures treated with screws, reported satisfactory outcomes after 10 years of follow-up, with one patient requiring extraction of the material, and one case of recurrent dislocation(20). Taking into account these findings in the literature, we recommend the described surgical technique for fragments corresponding to over 25% of the joint surface, to confirm that reduction is anatomical, with fixation using buttons, and thus reduce the potential complications associated with the use of screws.
In relation to the mentioned fixation difficulties, utilization of the arthroscopic button system described by Taverna et al. offers an alternative for fixing larger size fragments(4). Morash et al. published a detailed description of this fixation technique, highlighting key points of the procedure(21), such as starting with a posterior arthroscopy portal in a medial and upper position to keep the glenoid guide parallel to the glenoid surface, and drilling the anchorings for capsulolabral repair before reducing the bone fragment. Recently, Wafaisade et al. presented results of this arthroscopic button fixation technique, with a minimum follow-up of 6 months in 22 patients, recording a mean Constant value of 83.2 ± 16.7, with no complications or revision surgeries, and with consolidation of the fracture. At radiological follow-up, the mean displacement of the fragment (joint step) was 1.05 mm (0-4 mm)(22).
The described technique makes it possible to treat anterior glenoid fractures using a flexible device that reduces morbidity and potential discomfort associated with the use of screws. It is of interest to present arthroscopic fixation alternatives to manage fractures of this kind in a minimally invasive manner, while also treating associated soft tissue lesions at the same time. The use of a mechanical tensioning system affords rigidity, thus achieving adequate consolidation of the fragment(23). As limitations of the described technique, mention must be made of the fact that experience in shoulder arthroscopy is needed, as well as specific instruments that might not be widely available. On the other hand, the technique may not be adequate for comminuted fractures or fragments that are smaller in size than the arthroscopic button.
Conclusions
This study describes the case of a woman with a critical fracture fragment of the anterior glenoid labrum subjected to fully arthroscopic surgery and involving a non-rigid fixation method with the use of a button. The description of new fixation methods is still limited to technical notes, case reports and series with short periods of follow-up. Nevertheless, the described technique affords satisfactory clinical outcomes, is safe, and secures correct fracture consolidation.
Supplementary material
The video of the technique accompanying this article can be seen at (Video 1):
Figuras
Figure 1. Presurgical images of the lesion. A: computed tomography view (axial section) showing the displaced fracture of the anterior glenoid labrum; B: three-dimensional reconstruction confirming displacement and a fracture fragment size corresponding to 25% of the glenoid surface, using the perfect circle method with linear calculation; C: computed tomography view (sagittal section) of the glenoid cavity, confirming displacement of the fragment (9.5 mm).
Figure 2. Initial findings of right shoulder arthroscopy with the patient in left lateral decubitus, with visualization from the anterosuperior portal. A: osteochondral fracture fragment of the anterior glenoid labrum; B: reduction with glenoid hook guide from the posterior portal.
Figure 3. Shoulder arthroscopy images with the patient in lateral decubitus. A: fracture fragment with fixation using the arthroscopic button system; B: final anatomical reduction of the fragment.
Figure 4. Computed axial tomography view 6 months after the procedure. A: sagittal view with the fracture consolidated and stabilized with the arthroscopic button; B: three-dimensional reconstruction.
Tablas
Table 1. Tips and possible complications of the technique
Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The author Mauricio Largacha is a consultant to Smith and Nephew.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their center referred to the publication of patient information have been followed, and that all the patients included in the study have received sufficient information and have given written informed consent to participation in the study.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- From the start to the top: the history of knee osteotomies
- Clinical-functional and radiographic outcomes of medial valgus-producing tibial osteotomy
- Patellar tendinopathy: a practical consensus guide for choosing the best treatment
- Evolution of spinal endoscopy. Where do we come from and where are we going?
- Partial ruptures of the rotator cuff
- Arthroscopic core decompression of the femoral head with autologous stem cell placement as treatment for femoral head osteonecrosis
- Extraarticular plasty as sole maneuver in the correction of rotational instability due to rupture of the anterior cruciate ligament in an elderly patient
- Fully arthroscopic osteosynthesis with button placement in acute anterior glenoid fracture: a case report
- Arthroscopic visualization of the popliteal hiatus and localization of an intraarticular free body
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.