
Perioperative pain management in arthroscopy of the elbow
Manejo perioperatorio del dolor en artroscopia de codo
Introduction
Although arthroscopy of the elbow is technically demanding, in recent years it has become widely used and is both safe and effective in application to a growing number of disorders, thanks to improvement of the instruments, better knowledge of the anatomy, and training in complex surgical techniques(1,2).
The most common indications are the removal of foreign bodies in the joint, the treatment of lateral epicondylitis, the removal of synovial plicae, the management of osteochondritis dissecans, osteoarthrosis and septic arthritis, the treatment of post-traumatic stiffness and fracture osteosynthesis, as well as repair of the lateral ligament complex(3).
Perioperative pain of the elbow is generally considered to be less intense than in other locations such as the shoulder, though adequate management is required in order to ensure a shorter hospital stay and the early start of rehabilitation — thereby improving the postoperative outcomes and patient satisfaction, and reducing the hospital costs(4).
Despite this importance, the literature on the management of perioperative pain and the pain levels in elbow arthroscopy is very scarce.
The present study offers a narrative review of the available scientific literature on the different options for the management of perioperative pain in elbow arthroscopy, highlighting those which are most relevant, and providing a series of recommendations to guide the arthroscopist.
Importance of perioperative pain in arthroscopic surgery of the elbow
Inadequate perioperative pain control is associated to poorer long-term postoperative outcomes in elbow surgery(5). According to Desai et al.(6), there are two postoperative pain risk factors in elbow and shoulder surgery: preoperative pain and anticipated postoperative pain (APP) on day three — with preoperative pain being the most powerful pain predictor at 6 weeks post-surgery. Thus, the correct management of perioperative pain is of special relevance in the case of the elbow, due to its strong tendency to develop stiffness after surgery. Such stiffness, related to high levels of pain, does not allow the early start of exercises for improving articular movement, and can result in important functional loss(7).
A number of risk factors have been related to an increased need for postoperative rescue analgesia in upper limb surgeries(8):
- Surgery involving bone: in this regard, bone contains myelinated and non-myelinated afferent fibres, as well as nociceptors. These fibres in turn contain neuropeptides associated to the nociceptive process(9). In addition, bone involvement produces a higher increase in the levels of prostaglandin E2 compared with soft tissue involvement only(10).
- The length of surgery: longer surgeries imply more tissue damage and therefore a greater potential release of inflammatory mediators(8).
- Tourniquet use: the use of a tourniquet is generalised in elbow arthroscopy(11), but can be avoided in shorter procedures. Tourniquet-induced ischaemia causes tissue damage, and its severity depends on the duration of the ischaemia(12).
In addition, a number of patient-dependent factors have been described that can result in higher postoperative pain levels, including the female sex, overweight, depression and catastrophe ideation, smoking and alcohol abuse, loss of passive range of motion, anticipated preoperative pain and high preoperative pain levels(6). These predictors of increased postoperative pain can be identified preoperatively and are of great help in ensuring the best analgesic treatment for the patient.
With regard to the moment of maximum pain, the highest pain levels following elbow arthroscopy measured with the visual analogue scale (VAS) reportedly occur after 12 hours with the patient under resting conditions (VAS 41 ± 28), and at 24 hours post-surgery during physiotherapy (VAS 46 ± 29)(13).
Thus, in order to ensure good pain management and a favourable postoperative outcome, it is essential to consider the mentioned surgical and patient-dependent risk factors, with special attention to the moments in which the pain levels are highest.
reacae.29276.fs2111035en-table1.png
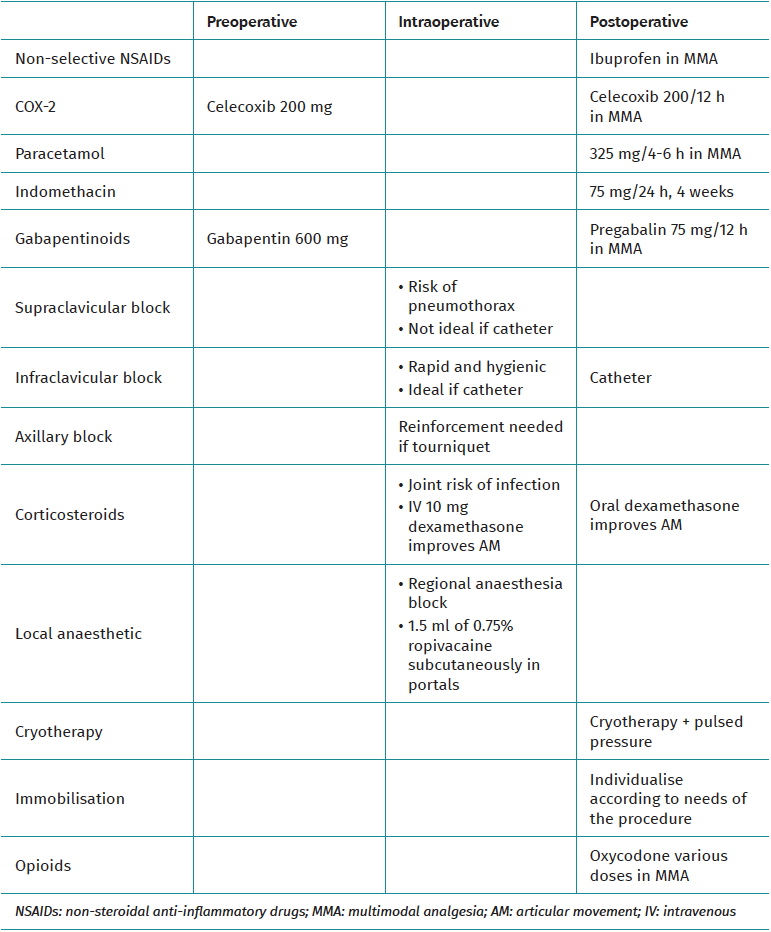
Table 1. Summary of therapeutic alternatives
Table 1 summarises the therapeutic options for the management of perioperative pain in elbow arthroscopy described below.
Assessment of pain in arthroscopy of the elbow
It is essential to quantify the postoperative pain levels using tools which are simple, reproducible and that contribute valid information, in order to ensure adequate pain management.
The most commonly used specific pain scales worldwide are the VAS(14) and the numeric pain scale, where 0 = no pain and 100 = maximum pain. However, these are simple unidimensional scales that do not address either the aetiology or the complexity of pain. The Brief Pain Inventory (previously known as the Brief Pain Questionnaire) is a multidimensional scale; consequently, and in contrast to the previously mentioned scales, it allows more concrete evaluation of the characteristics of the pain. Although originally developed to assess cancer pain, it is currently also used to score non-oncological pain, and both its brief and long versions have been validated in Spanish(15).
There are elbow assessment scales that include specific sections referred to pain. These instruments include the Oxford Elbow Score, which compiles sociological, functional and pain data after surgery, scored from 0-100 points, and which has been found to be closely correlated to the VAS(16). The Mayo Elbow Performance Score (MEPS) in turn collects information on pain, range of motion, stability and function of the elbow — the score related to the section on pain being between 0 and 45 points out of a total of 100 possible points(17).
Preoperative management
Preventive analgesia is understood as an intervention carried out before the pain stimulus appears, with the aim of blocking peripheral and central nociception, and maintaining the block from the intraoperative period to the postoperative interval. The main aims of preventive analgesia are to reduce acute pain after tissue trauma, prevent the modulation exerted by the central nervous system in relation to the pain, and inhibit the persistence of postoperative pain, avoiding the development of chronic pain(18). Preventive analgesia is still subject to controversy, but has been successfully used in terms of efficacy and safety in other disciplines and even in arthroplasty surgery of the knee and hip. Evidence on its utilisation in elbow arthroscopy is limited, however(19).
Non-steroidal anti-inflammatory drugs (NSAIDs)
The NSAIDs are among the most widely used drugs for reducing pain. By inhibiting the action of the enzymes COX-2 and COX-1, these drugs lower prostaglandin production, thereby reducing inflammation and pain. The use of non-selective COX-2 inhibitors for preventive analgesia is currently only testimonial, since in the last 15 years they have been replaced by more effective agents(19). Although no specific evaluation has been made of the use of selective COX-2 inhibitors in elbow arthroscopy, their utilisation is widely accepted in arthroscopic surgery(20) and even in upper limb surgery(21). In any case, and regardless of the type of surgery involved, the selective COX-2 inhibitors when administered preoperatively afford positive effects in terms of the postoperative pain levels, opioid consumption and the duration of hospital stay(19).
Gabapentinoids
Gabapentin and pregabalin are structural analogues of gamma-aminobutyric acid (GABA), and traditionally have been used for the control of neuropathic pain. However, in the last two decades many articles have suggested that their administration as preventive analgesia affords benefits both in terms of opioid consumption and as regards the pain scores(22). These effects have also been demonstrated in arthroscopic surgery with 600 mg of gabapentin administered two hours before surgery, as evidenced by Huang et al.(23), though the specific efficacy of this drug in elbow arthroscopy has not been evaluated to date. It is also known that gabapentin administered in combination with other analgesic drugs may exert a synergic effect — though this likewise has not been evaluated in elbow arthroscopy(24).
Intraoperative management
Traditionally, elbow arthroscopy has been performed under general anaesthesia, with the advantage of being able to perform a neurological exploration in the immediate postoperative period(25). However, the regional anaesthesia techniques have gradually displaced general anaesthesia due to their fewer adverse effects (e.g. nausea and drowsiness), with better control of postoperative pain — reducing opioid consumption in the immediate postoperative period and up to 90 days after elbow surgery(26,27). At present, ultrasound-guided techniques are the gold standard for most nerve blocks in surgery of the upper limb, affording improved precision with a decrease in complications versus block procedures guided by electrostimulation and anatomical references. In addition, they allow catheter placement for perioperative pain control(28), facilitating painless early mobilisation, which is of particular interest in some elbow surgeries(29).
Interscalene block
Interscalene block affords good anaesthetic coverage of the shoulder and the lateral aspect of the arm. However, although it has been successfully used in surgery of the elbow(30), it is not appropriate for surgeries distal to the shoulder, because as a rule and using traditional techniques, the inferior trunk of the plexus arising from roots C8 and T1 is not blocked(31). This situation can be solved by using a combined technique, for example, an AXIS block(32) (double axillary and interscalene block) — though there are other alternative approaches for blocking the plexus in arthroscopic surgery of the elbow that are more appropriate.
Supraclavicular block
This is the oldest of the plexus block techniques, having been described in 1911(33). The aim is to block all the plexus trunks within the fascia that includes the subclavian artery, thereby affording a rapid effect with relatively low volumes of local anaesthetic(26). Supraclavicular block is able to cover the territory from the middle third of the humerus to the hand, and is useful when a tourniquet is required. However, it is not the technique of choice for placing a continuous analgesia catheter, due to the associated risk of pneumothorax — despite the fact that the use of ultrasound greatly reduces this risk(34).
Infraclavicular block
The aim of this technique is to deposit the local anaesthetic in the plexus proximal to the point of emergence of the musculocutaneous, axillary and medial brachial cutaneous nerves, affording a very high success rate with a single puncture(26). Many access routes for performing this block have been described, though the use of ultrasound clearly improves precision(35). Furthermore, infraclavicular block is faster and has a lower number of complications (e.g. pneumothorax) than supraclavicular block, with similar success rates(36). It is important to note that this block, in addition to affording effective anaesthesia for elbow arthroscopy and for the use of a tourniquet, is also adequate for the placement of a catheter for continuous postoperative analgesia, since it is not located in a mobile segment of the arm and is more hygienic than the axillary region(37).
Axillary block
Axillary block seeks an anaesthetic effect by acting upon the terminal branches of the plexus, and is the most widely used technique for surgeries distal to the shoulder — including the elbow(38). It affords excellent anaesthesia with a very good safety profile — particularly when performed under ultrasound guidance — since the block zone is located away from the neck structures(39). The disadvantages of this technique are summarised below: 1) the musculocutaneous nerve requires anaesthetic reinforcement if a tourniquet is to be used, since this level is not blocked; 2) the technique is contraindicated in patients unable to perform the abduction and external rotation of the shoulder required to have good access to the axilla; 3) in the absence of sensory or motor block of the shoulder, patient comfort may be adversely affected in this abduction position; and 4) the technique is less adequate than infraclavicular block for placing a catheter for continuous postoperative analgesia, due to the abovementioned reasons. As a point of controversy, Wada et al.(13) recorded no differences in the postoperative VAS score between patients subjected to elbow arthroscopy under general anaesthesia and single-puncture axillary block and a control group operated upon under general anaesthesia with the preoperative subcutaneous injection of 1.5 ml of 0.75% ropivacaine in each portal.
Local anaesthetics and adjuvants
The choice of local anaesthetic used in regional anaesthesia is determined by the length of surgery, the required degree of motor block, the need to perform an exploration of nerve function in the immediate postoperative period, and the postoperative analgesia requirements(26). Lidocaine and mepivacaine are very widely used thanks to their rapid action and potency. However, the effects are short lasting, and so these drugs are best suited for short surgeries(40). Bupivacaine and ropivacaine are slower acting but afford longer lasting effects, and so are the drugs of choice when postoperative analgesia is required. Levobupivacaine is an isomer of bupivacaine but with lesser cardiotoxicity, in the same way as ropivacaine(41).
In relation to the volume of anaesthetic, the doses used when performing blocks guided by anatomical references were high because large volumes (42 to 80 ml) afforded greater anaesthesia success rates(42). However, with the use of ultrasound-guided techniques, the doses have decreased to between 1-7 ml/nerve by improving precision in depositing the anaesthetic on target(43,44).
There is abundant information on the use of adjuvant drugs which when administered during nerve block are able to improve some of the characteristics of the block. One of these drug substances is clonidine. When administered in the supraclavicular plexus under ultrasound guidance together with bupivacaine, clonidine has been seen to shorten the onset of block, prolong sensory and motor block, and also afford postoperative analgesia as well as mild sedation, with few side effects(45,46). When administered at perineural level in infraclavicular block under ultrasound guidance, dexamethasone — a synthetic corticosteroid — has been shown to afford a 19-22% longer duration of motor and sensory block, as well as longer postoperative analgesia versus intravenous dexamethasone(47) — the effect being equivalent with perineural doses of 2, 5 and 8 mg(48). It has also been reported that fentanyl — a major opioid — administered together with bupivacaine during supraclavicular block, prolongs the effect of block without adverse effects(49), and could even shorten the time to block versus clonidine(50). Magnesium sulfate has also been widely studied as an adjuvant, and when administered together with lidocaine in infraclavicular block or with ropivacaine in axillary block, it prolongs the anaesthetic and analgesic effect up to 12 hours after surgery, without adverse events(51,52).
Catheter for continuous infusion
Pain control after arthroscopic surgery of the elbow is crucial, mainly because of the benefits afforded by the early mobilisation of this particular joint, which has a clear tendency to develop stiffness. However, in some cases such early mobilisation is only possible in patients who carry a catheter for the continuous administration of anaesthetic in the brachial plexus. The use of such catheters for the continuous infusion of anaesthetics as postoperative pain control measure in elbow surgery has been seen to be very effective in the first 24-48 postoperative hours(53). The advantages of this approach versus isolated plexus block are a longer duration of block, reduction of the postoperative pain levels, lesser opioid consumption, and increased patient satisfaction(54). The procedures that benefit most from the use of catheters for continuous analgesia are arthrolysis and the arthroscopic management of osteoarthrosis — allowing the use of continuous mobilisation devices or physiotherapy without pain(55,56). Catheter use has been described on an in-hospital basis, though also in the ambulatory setting, with good results in terms of pain control, opioid use, side effects and cost-effectiveness(57,58). The causes of catheter failure include problems with the insertion technique used, anatomical variants of the patient, the administration of insufficient medication, and catheter displacement. In this regard, Quast et al.(59) compared the two most frequently used block sites in arthroscopic surgery of the elbow: infraclavicular and axillary. The authors compared 119 infraclavicular catheters and 209 axillary catheters, and recorded no differences in the early postoperative (first 24 hours) failure rate: 6.7% in the infraclavicular catheter group versus 6.2% in the case of the axillary catheters (p = 0.449).
Corticosteroids
There are descriptions of the intraarticular administration of corticosteroids, particularly in patients with stiffness, but the risk of infection outweighs the possible benefits of intraarticular dosing. Nelson et al.(60) recorded a 14% and 4.9% incidence of superficial and deep infections, respectively, in patients who had been treated intraoperatively with intraarticular corticosteroids, versus 2% and 4%, respectively, in subjects that had not received intraarticular corticosteroids (p < 0.0001). The intravenous administration of 10 mg of dexamethasone followed by oral dexamethasone during 6 days after elbow surgery has also been reported, with no improvement of the pain versus the control group, but with significant improvement of articular movement(61).
Local anaesthetic infiltration
The application of local anaesthetic in the portals is a common practice in arthroscopic surgery, but not in the specific case of the elbow. Nevertheless, it has been described mainly when the procedure is carried out under general anaesthesia without nerve block(62). In their clinical trial, Wada et al.(13) concluded that the administration of 1.5 ml of 0.75% ropivacaine subcutaneously in each portal before insufflation of the tourniquet afforded adequate pain control in a group of patients operated upon under general anaesthesia versus a control group in which axillary block was added to general anaesthesia.
Postoperative management
Cryotherapy
The application of cold has a number of physiological effects, such as the reduction of skin temperature and nerve conduction, and moreover decreases tissue metabolism — avoiding the appearance of cytokines and their pro-inflammatory effects(63). With regard to elbow surgery, Yu et al. demonstrated that the application of cryotherapy and pressure at 30-second intervals reduced the pain levels under resting conditions and during activity until the seventh postoperative day, and furthermore led to a decrease in opioid use with respect to a control group(64).
Immobilisation versus passive continuous mobilisation systems
In soft tissue surgery such as the arthroscopic treatment of epicondylitis or synovial plicae, a brief period of patient immobilisation is generally advised as an analgesic measure, followed by a rehabilitation plan to avoid stiffness and gradually recover muscle strength(62). In contrast, procedures intended to increase joint range of motion, such as arthroscopic arthrolysis or the arthroscopic treatment of osteoarthrosis, often benefit from the use of passive continuous mobilisation systems that require good pain control in order to improve patient tolerance during the first postoperative days(55,57). Even in patients with very severe elbow flexion contractures, there have been descriptions of the postoperative use of orthoses in extension during a variable number of days in order to avoid early relapse of flexion stiffness(60).
Patient-controlled analgesia (PCA)
Patient-controlled analgesia (PCA) systems allow the patient to personally decide when and how much analgesia is needed, according to the level of pain experienced. Such systems are widely used in certain settings (such as the United States), and represent the most common form of postoperative opioid administration(65). Although opioids may be very effective in terms of pain control, the reported incidence of adverse events (e.g. respiratory depression, nausea, vomiting and drowsiness) can result in a high dropout rate even if good pain control cannot be achieved without them(66). In elbow surgery, Lee et al. concluded that a multimodal analgesia regimen affords pain control equivalent to that obtained with the administration of oxycodone using a PCA system, but with a lower incidence of complications(5). In elbow surgery, use has also been made of PCA systems that instead of administering opioids via the intravenous route, deliver a local anaesthetic through a catheter, as has already been commented above, though in this case controlled by the patient. This is the so-called PCRA (patient-controlled regional analgesia), and has been shown to be useful in the first stages of postoperative recovery administering 0.4% ropivacaine(67).
Postoperative multimodal analgesia (MMA)
Multimodal analgesia (MMA) refers to the use of different therapeutic approaches, combined and/or in sequence, aimed at securing adequate pain control while avoiding side effects and complications derived from the use of such approaches. MMA includes a number of options, some of which have already been commented, such as preventive analgesia, nerve blocks, and the intraoperative and postoperative use of drugs. One of the key aspects of MMA is the use of drugs that act upon different receptors implicated in nociception, seeking a sum of effects or synergic action between them — thereby allowing for a decrease in the administered dose of each individual drug(68).
The most commonly used drugs in postoperative MMA are NSAIDs — both selective and non-selective COX-2 inhibitors — corticosteroids, antiepileptic agents such as gabapentin and pregabalin, antidepressants and opioids. The combined use of these substances blocks the nociceptive pathways at various points, affording a greater analgesic effect, rather than when blocking a single pathway(69). Such a multimodal approach is better able to control perioperative pain, and special attention should focus on those patients with a greater risk of suffering intense pain in the postoperative phase.
There is extensive experience with MMA in surgery of the knee, hip and even shoulder, but few studies in the literature have addressed elbow surgery, and specifically arthroscopic surgery of the elbow; as a result, no standardised MMA protocol has been established for this type of surgery.
The MMA regimen described by Cruz et al.(57) following complex arthroscopic surgery of the elbow includes 75 mg of indomethacin a day during three weeks, 10 mg of oxycodone every 12 hours, and a combination of 325 mg of paracetamol with 5 mg of oxycodone every 4-6 hours, depending on the patient needs. In turn, the MMA protocol described by Lee et al.(5) after upper limb surgery comprises 10 mg of oxycodone every 12 hours for one week, 650 mg of paracetamol every 8 hours for two weeks and, from the first postoperative day, 800 mg of ibuprofen + 200 mg of celecoxib + 75 mg of pregabalin, all administered every 12 hours. With this MMA protocol, Lee et al. achieved better pain control under resting conditions and during activity versus a control group with PCA system — though the difference was not statistically significant. The patients in the PCA group required more rescue analgesia and had a higher incidence of adverse events related to opioid consumption than the patients in the MMA group — the differences being statistically significant in both cases (p = 0.014 and 0.018, respectively).
Non-steroidal anti-inflammatory drugs and heterotopic ossification
Heterotopic ossification is a cause of pain and often appears after elbow trauma surgery. The incidence reaches 30-37% in such procedures, with a functional impact upon 20% of the patients(70). In the case of fractures, the use of NSAIDs for the prevention of heterotopic ossification implies an increased risk of pseudoarthrosis of the fracture point(71).
In the postoperative period of arthroscopic surgery of the elbow with osteoarthrosis or stiffness(55), it is common to administer NSAIDs such as indomethacin at a dose of 75 mg/24 hours during four weeks for the prevention of heterotopic ossification, as well as for pain control — though this practice is still subject to controversy(72).
Conclusions
- In relation to pain control following arthroscopic surgery of the elbow, the selective COX-2 inhibitors when administered preoperatively afford positive effects in terms of the postoperative pain levels and opioid consumption, and moreover shorten hospital stay.
- Ultrasound-guided regional anaesthesia techniques have displaced general anaesthesia thanks to their greater capacity to control pain, with a lesser incidence of adverse events such as nausea and drowsiness.
- The blocks of choice in elbow arthroscopy are the axillary and infraclavicular blocks — the latter being preferred if the postoperative continuous infusion of analgesia using a catheter is planned.
- There are adjuvants such as clonidine, dexamethasone, fentanyl or magnesium sulfate which, when administered together with the local anaesthetic used for performing the block, can improve the characteristics of the latter by shortening the time to onset of the block or prolonging its effect, in order to afford better postoperative pain control.
- Cryotherapy and pressure applied in pulses at intervals can reduce pain up to day 7 after surgery.
- PCA systems are very effective in controlling pain, but the adverse events of the administered opioids often cause patients to abandon the treatment.
- MMA should be the cornerstone on which to base the management of perioperative pain, though its use in elbow arthroscopy has not been protocolised to date.
Tablas
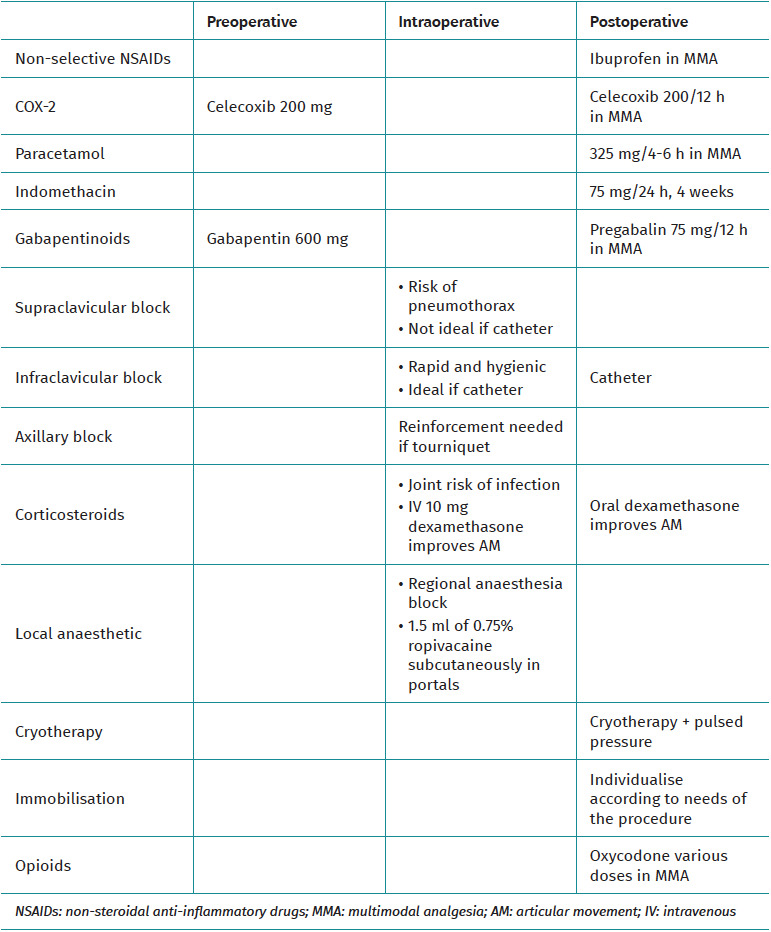
Table 1. Summary of therapeutic alternatives
Información del artículo
Cita bibliográfica
Ethical responsibilities
Conflicts of interest. The authors state that they have no conflicts of interest.
Financial support. This study has received no financial support.
Protection of people and animals. The authors declare that this research has not involved human or animal experimentation.
Data confidentiality. The authors declare that the protocols of their work centre referred to the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Descargar artículo:
Licencia:
Este contenido es de acceso abierto (Open-Access) y se ha distribuido bajo los términos de la licencia Creative Commons CC BY-NC-ND (Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional) que permite usar, distribuir y reproducir en cualquier medio siempre que se citen a los autores y no se utilice para fines comerciales ni para hacer obras derivadas.
Comparte este contenido
En esta edición
- The importance of pain control
- Learning from pain to make the patient feel better
- Perioperative pain management in arthroscopic surgery of the shoulder
- Perioperative pain management in arthroscopy of the elbow
- Perioperative analgesia in arthroscopic surgery of the wrist and hand
- Perioperative analgesia in arthroscopy of the hip
- Perioperative analgesia in arthroscopic surgery of the knee
- Perioperative pain management in arthroscopy of the ankle
- Postoperative neuropathic pain in traumatology
- Capsaicin 179 mg patch application technique
- Type 3 SLAP: bucket handle tear
Más en PUBMED
Más en Google Scholar
Más en ORCID

Revista Española de Artroscopia y Cirugía Articular está distribuida bajo una licencia de Creative Commons Reconocimiento-NoComercial-SinObraDerivada 4.0 Internacional.